

Health Gains and Financial Protection from Pneumococcal Vaccination and Pneumonia Treatment in Ethiopia: Results from an Extended Cost-Effectiveness Analysis
- PMID: 26650078
- PMCID: PMC4674114
- DOI: 10.1371/journal.pone.0142691
Health Gains and Financial Protection from Pneumococcal Vaccination and Pneumonia Treatment in Ethiopia: Results from an Extended Cost-Effectiveness Analysis
Abstract
Background: Pneumonia and pneumococcal disease cause a large disease burden in resource-constrained settings. We pursue an extended cost-effectiveness analysis (ECEA) of two fully publicly financed interventions in Ethiopia: pneumococcal vaccination for newborns and pneumonia treatment for under-five children in Ethiopia.
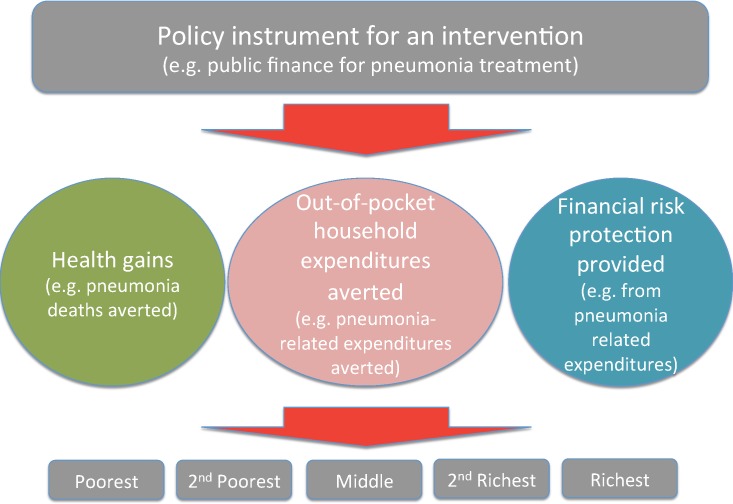
Methods: We apply ECEA methods and estimate the program impact on: (1) government program costs; (2) pneumonia and pneumococcal deaths averted; (3) household expenses related to pneumonia/pneumococcal disease treatment averted; (4) prevention of household medical impoverishment measured by an imputed money-metric value of financial risk protection; and (5) distributional consequences across the wealth strata of the country population. Available epidemiological and cost data from Ethiopia are applied and the two interventions are assessed separately at various incremental coverage levels.
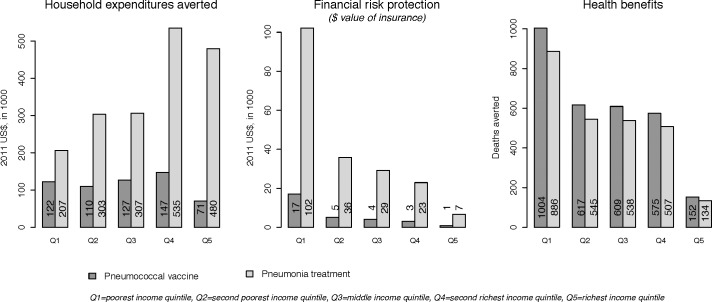
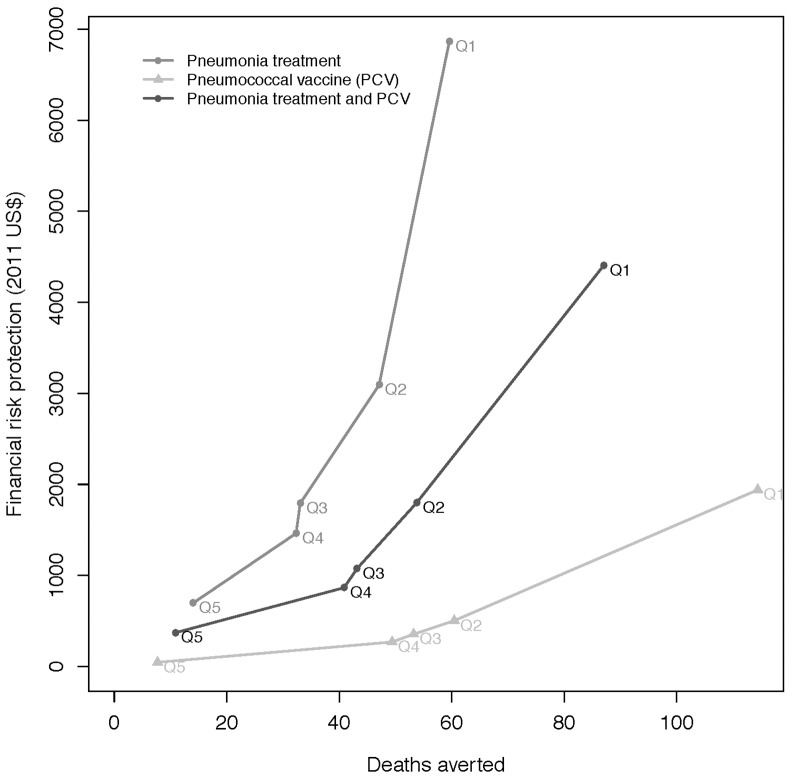
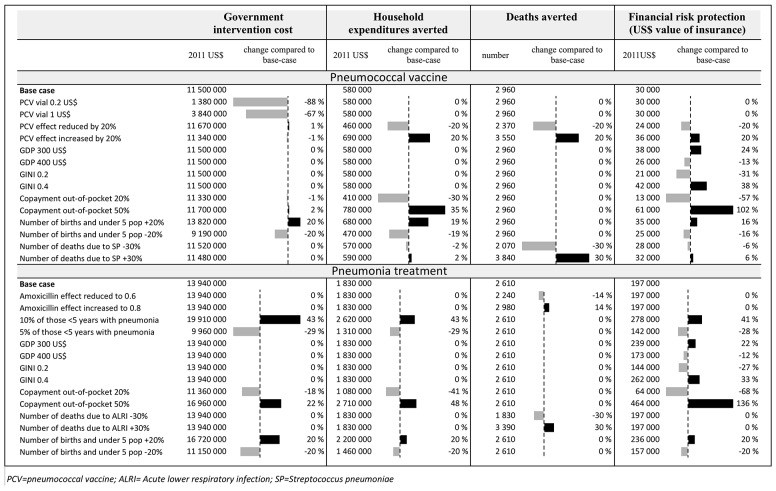
Results: Scaling-up pneumococcal vaccines at around 40% coverage would cost about $11.5 million and avert about 2090 child deaths annually, while a 10% increase of pneumonia treatment to all children under 5 years of age would cost about $13.9 million and avert 2610 deaths annually. Health benefits of the two interventions publicly financed would be concentrated among the bottom income quintile, where 30-40% of all deaths averted would be expected to occur in the poorest quintile. In sum, the two interventions would eliminate a total of $2.4 million of private household expenditures annually, where the richest quintile benefits from around 30% of the total private expenditures averted. The financial risk protection benefits would be largely concentrated among the bottom income quintile. The results are most sensitive to variations in vaccine price, population size, number of deaths due to pneumonia, efficacy of interventions and out-of-pocket copayment share.
Conclusions: Vaccine and treatment interventions for children, as shown with the illustrative examples of pneumococcal vaccine and pneumonia treatment, can bring large health and financial benefits to households in Ethiopia, most particularly among the poorest socio-economic groups.
Conflict of interest statement
Figures
Similar articles
-
Health gains and financial risk protection afforded by public financing of selected interventions in Ethiopia: an extended cost-effectiveness analysis.Lancet Glob Health. 2015 May;3(5):e288-96. doi: 10.1016/S2214-109X(14)70346-8. Lancet Glob Health. 2015. PMID: 25889470
-
Economic evaluation of childhood 7-valent pneumococcal conjugate vaccination in Korea.J Manag Care Pharm. 2010 Jan-Feb;16(1):32-45. doi: 10.18553/jmcp.2010.16.1.32. J Manag Care Pharm. 2010. PMID: 20044845 Free PMC article.
-
Public finance of rotavirus vaccination in India and Ethiopia: an extended cost-effectiveness analysis.Vaccine. 2013 Oct 1;31(42):4902-10. doi: 10.1016/j.vaccine.2013.07.014. Epub 2013 Jul 16. Vaccine. 2013. PMID: 23871824
-
Health Gains and Financial Risk Protection Afforded by Treatment and Prevention of Diarrhea and Pneumonia in Ethiopia: An Extended Cost-Effectiveness Analysis.In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 19. In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 19. PMID: 27227233 Free Books & Documents. Review.
-
The pharmacoeconomics of pneumococcal conjugate vaccines in Latin America.Vaccine. 2011 Sep 14;29 Suppl 3:C35-42. doi: 10.1016/j.vaccine.2011.06.095. Vaccine. 2011. PMID: 21896351 Review.
Cited by
-
Incorporating Equity Concerns in Cost-Effectiveness Analyses: A Systematic Literature Review.Pharmacoeconomics. 2022 Jan;40(1):45-64. doi: 10.1007/s40273-021-01094-7. Epub 2021 Oct 29. Pharmacoeconomics. 2022. PMID: 34713423
-
Estimating the distribution of morbidity and mortality of childhood diarrhea, measles, and pneumonia by wealth group in low- and middle-income countries.BMC Med. 2018 Jul 4;16(1):102. doi: 10.1186/s12916-018-1074-y. BMC Med. 2018. PMID: 29970074 Free PMC article.
-
Why vaccines matter: understanding the broader health, economic, and child development benefits of routine vaccination.Hum Vaccin Immunother. 2020 Aug 2;16(8):1900-1904. doi: 10.1080/21645515.2019.1708669. Epub 2020 Jan 24. Hum Vaccin Immunother. 2020. PMID: 31977283 Free PMC article.
-
Costs incurred by caregivers of under-five inpatients with community-acquired pneumonia at a university hospital in south-western Ethiopia.S Afr J Infect Dis. 2019 Jul 29;34(1):109. doi: 10.4102/sajid.v34i1.109. eCollection 2019. S Afr J Infect Dis. 2019. PMID: 34485450 Free PMC article.
-
Reducing regional health inequality: a sub-national distributional cost-effectiveness analysis of community-based treatment of childhood pneumonia in Ethiopia.Int J Equity Health. 2021 Jan 6;20(1):9. doi: 10.1186/s12939-020-01328-8. Int J Equity Health. 2021. PMID: 33407559 Free PMC article.
References
-
- UN Inter-agency Group for Child Mortality Estimation (2013) Levels & Trends in Child Mortality: Report 2013.
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2095–2128. 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- Institute for Health Metrics and Evaluation (2014) Global Burden of Disease study 2010. Seattle.
-
- World Bank, World Development Indicators (2014): The World Bank: Washington, DC.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
