

Effect of abatacept on the immunogenicity of 23-valent pneumococcal polysaccharide vaccination (PPSV23) in rheumatoid arthritis patients
- PMID: 26653668
- PMCID: PMC4675027
- DOI: 10.1186/s13075-015-0863-3
Effect of abatacept on the immunogenicity of 23-valent pneumococcal polysaccharide vaccination (PPSV23) in rheumatoid arthritis patients
Abstract
Introduction: Patients with rheumatoid arthritis (RA) treated with abatacept (ABT) are at increased risk for vaccine-preventable infections. The aim of the present study is to evaluate the humoral response to 23-valent pneumococcal polysaccharide (PPSV23) vaccination in RA patients receiving ABT.
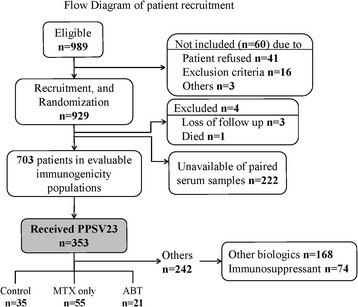
Methods: The immunogenicity study was nested within a randomized, double-blind placebo-controlled study, designed to evaluate the efficacy of the PPSV23. PPSV23 was given to 111 RA patients, who were classified into three groups: RA control (n = 35), methotrexate (MTX) alone (n = 55), and ABT (n = 21). Before and 4-6 weeks after vaccination, we measured the patients' concentrations of antibodies against pneumococcal serotypes 6B and 23F using an enzyme-linked immunosorbent assay and determined their antibody functionality using a multiplexed opsonophagocytic killing assay, reported as the opsonization index (OI).
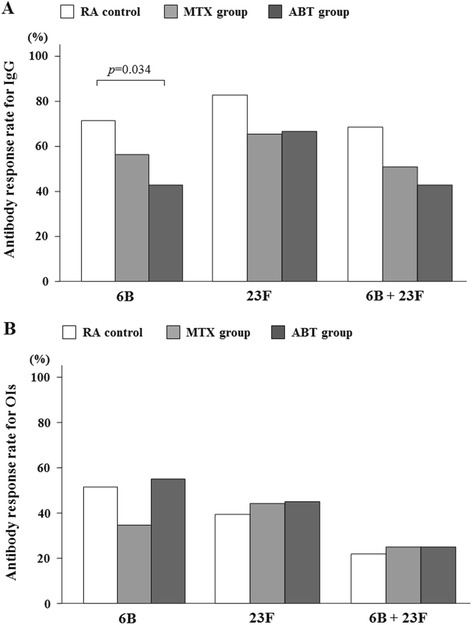
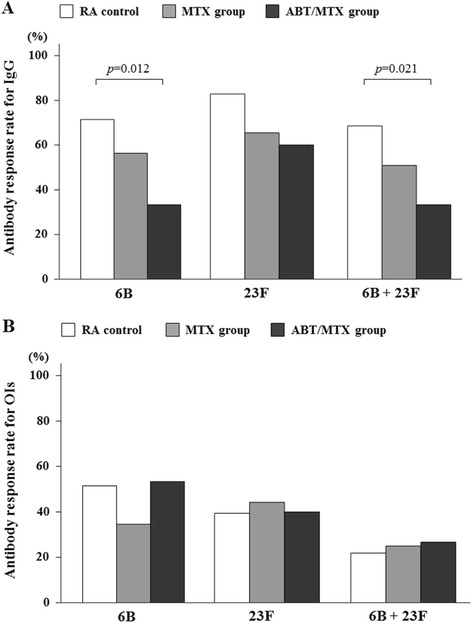
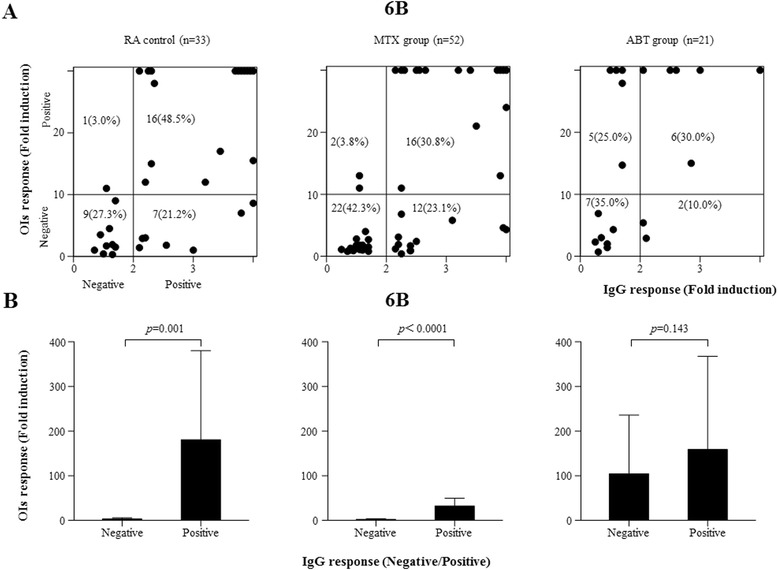
Results: The pneumococcal serotype-specific IgG concentrations and OIs were both significantly increased in all treatment groups in response to PPSV23 vaccination. In the ABT group, the IgG responses for the 6B serotype were lower compared with those in the MTX alone or control groups, whereas the OI responses were similar to those in the other two groups. In a subgroup analysis, the pneumococcal serotype-specific IgG responses were significantly lower in both serotypes (6B and 23F) in the ABT/MTX group; however, the OI responses in the ABT group were not different from the control group. There was no association between the pneumococcal serotype-specific IgG and OI responses for the 6B serotype in patients receiving ABT in contrast to the control or MTX alone patients. No severe adverse effects were observed in any of the treatment groups.
Conclusions: OI responses indicate antibody functionality rather than simply their amount, so the similarity of these measurements between all three groups suggests that RA patients receiving ABT still benefit from receiving the PPSV23 vaccination, even though they produce less IgG in response to it. The results suggest an influence of ABT on the humoral response to PPSV23 vaccination under MTX treatment; however, preserved opsonin responses are expected in RA patients treated with ABT plus MTX.
Trial registration: University Hospital Medical Information Network Clinical Trials Registry: UMIN000009566. Registered 12 December 2012.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
