

Clinical course of untreated cerebral cavernous malformations: a meta-analysis of individual patient data
- PMID: 26654287
- PMCID: PMC4710581
- DOI: 10.1016/S1474-4422(15)00303-8
Clinical course of untreated cerebral cavernous malformations: a meta-analysis of individual patient data
Abstract
Background: Cerebral cavernous malformations (CCMs) can cause symptomatic intracranial haemorrhage (ICH), but the estimated risks are imprecise and predictors remain uncertain. We aimed to obtain precise estimates and predictors of the risk of ICH during untreated follow-up in an individual patient data meta-analysis.
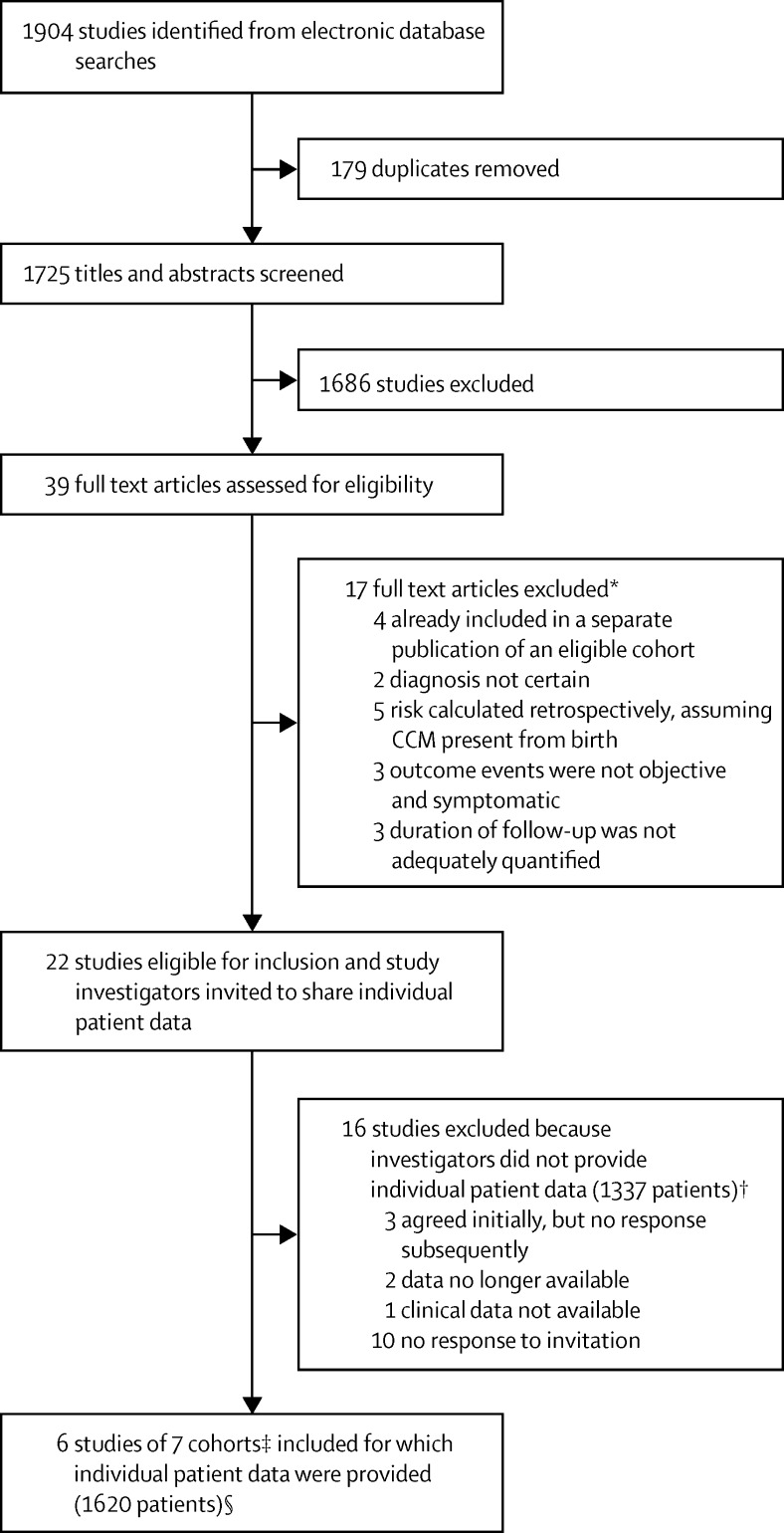
Methods: We invited investigators of published cohorts of people aged at least 16 years, identified by a systematic review of Ovid MEDLINE and Embase from inception to April 30, 2015, to provide individual patient data on clinical course from CCM diagnosis until first CCM treatment or last available follow-up. We used survival analysis to estimate the 5-year risk of symptomatic ICH due to CCMs (primary outcome), multivariable Cox regression to identify baseline predictors of outcome, and random-effects models to pool estimates in a meta-analysis.
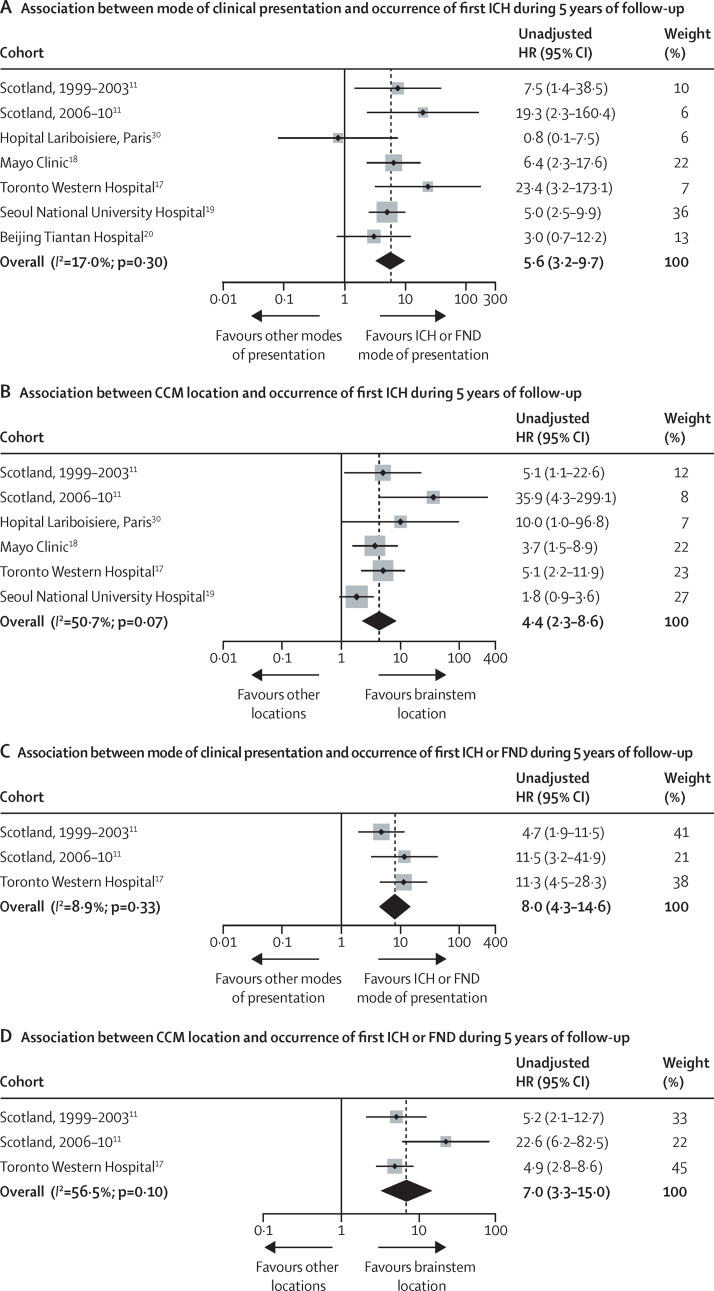
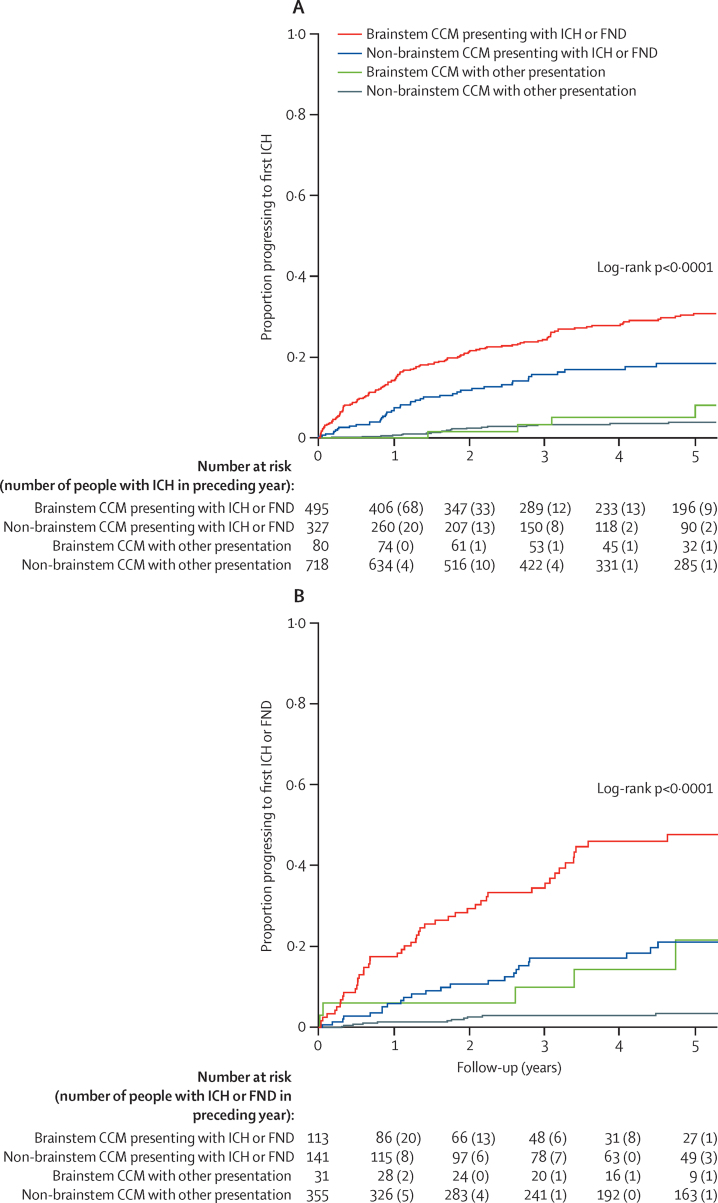
Findings: Among 1620 people in seven cohorts from six studies, 204 experienced ICH during 5197 person-years of follow-up (Kaplan-Meier estimated 5-year risk 15·8%, 95% CI 13·7-17·9). The primary outcome of ICH within 5 years of CCM diagnosis was associated with clinical presentation with ICH or new focal neurological deficit (FND) without brain imaging evidence of recent haemorrhage versus other modes of presentation (hazard ratio 5·6, 95% CI 3·2-9·7) and with brainstem CCM location versus other locations (4·4, 2·3-8·6), but age, sex, and CCM multiplicity did not add independent prognostic information. The 5-year estimated risk of ICH during untreated follow-up was 3·8% (95% CI 2·1-5·5) for 718 people with non-brainstem CCM presenting without ICH or FND, 8·0% (0·1-15·9) for 80 people with brainstem CCM presenting without ICH or FND, 18·4% (13·3-23·5) for 327 people with non-brainstem CCM presenting with ICH or FND, and 30·8% (26·3-35·2) for 495 people with brainstem CCM presenting with ICH or FND.
Interpretation: Mode of clinical presentation and CCM location are independently associated with ICH within 5 years of CCM diagnosis. These findings can inform decisions about CCM treatment.
Funding: UK Medical Research Council, Chief Scientist Office of the Scottish Government, and UK Stroke Association.
Copyright © 2016 Horne et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Prognosis of cerebral cavernomas: on to treatment decisions.Lancet Neurol. 2016 Feb;15(2):129-130. doi: 10.1016/S1474-4422(15)00340-3. Epub 2015 Dec 2. Lancet Neurol. 2016. PMID: 26654286 No abstract available.
References
-
- Greving JP, Wermer MJH, Brown RD., Jr Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014;13:59–66. - PubMed
-
- Vernooij MW, Ikram MA, Tanghe HL. Incidental findings on brain MRI in the general population. N Engl J Med. 2007;357:1821–1828. - PubMed
-
- Rigamonti D, Drayer BP, Johnson PC, Hadley MN, Zabramski J, Spetzler RF. The MRI appearance of cavernous malformations (angiomas) J Neurosurg. 1987;67:518–524. - PubMed
-
- Brown RD, Wiebers DO, Torner JC, O'Fallon WM. Frequency of intracranial hemorrhage as a presenting symptom and subtype analysis: a population-based study of intracranial vascular malformations in Olmsted County, Minnesota. J Neurosurg. 1996;85:29–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
