

A numerical similarity approach for using retired Current Procedural Terminology (CPT) codes for electronic phenotyping in the Scalable Collaborative Infrastructure for a Learning Health System (SCILHS)
- PMID: 26655696
- PMCID: PMC4676189
- DOI: 10.1186/s12911-015-0223-x
A numerical similarity approach for using retired Current Procedural Terminology (CPT) codes for electronic phenotyping in the Scalable Collaborative Infrastructure for a Learning Health System (SCILHS)
Abstract
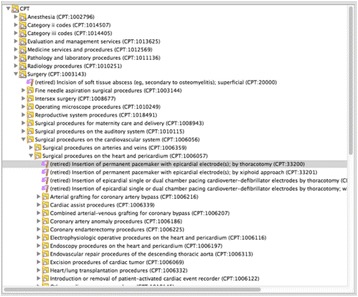
Background: Interoperable phenotyping algorithms, needed to identify patient cohorts meeting eligibility criteria for observational studies or clinical trials, require medical data in a consistent structured, coded format. Data heterogeneity limits such algorithms' applicability. Existing approaches are often: not widely interoperable; or, have low sensitivity due to reliance on the lowest common denominator (ICD-9 diagnoses). In the Scalable Collaborative Infrastructure for a Learning Healthcare System (SCILHS) we endeavor to use the widely-available Current Procedural Terminology (CPT) procedure codes with ICD-9. Unfortunately, CPT changes drastically year-to-year - codes are retired/replaced. Longitudinal analysis requires grouping retired and current codes. BioPortal provides a navigable CPT hierarchy, which we imported into the Informatics for Integrating Biology and the Bedside (i2b2) data warehouse and analytics platform. However, this hierarchy does not include retired codes.
Methods: We compared BioPortal's 2014AA CPT hierarchy with Partners Healthcare's SCILHS datamart, comprising three-million patients' data over 15 years. 573 CPT codes were not present in 2014AA (6.5 million occurrences). No existing terminology provided hierarchical linkages for these missing codes, so we developed a method that automatically places missing codes in the most specific "grouper" category, using the numerical similarity of CPT codes. Two informaticians reviewed the results. We incorporated the final table into our i2b2 SCILHS/PCORnet ontology, deployed it at seven sites, and performed a gap analysis and an evaluation against several phenotyping algorithms.
Results: The reviewers found the method placed the code correctly with 97 % precision when considering only miscategorizations ("correctness precision") and 52 % precision using a gold-standard of optimal placement ("optimality precision"). High correctness precision meant that codes were placed in a reasonable hierarchal position that a reviewer can quickly validate. Lower optimality precision meant that codes were not often placed in the optimal hierarchical subfolder. The seven sites encountered few occurrences of codes outside our ontology, 93 % of which comprised just four codes. Our hierarchical approach correctly grouped retired and non-retired codes in most cases and extended the temporal reach of several important phenotyping algorithms.
Conclusions: We developed a simple, easily-validated, automated method to place retired CPT codes into the BioPortal CPT hierarchy. This complements existing hierarchical terminologies, which do not include retired codes. The approach's utility is confirmed by the high correctness precision and successful grouping of retired with non-retired codes.
Figures



References
-
- Hadley M, McCready R, Delano D, Devarajan S. Assessing the Feasibility of Meaningful Use Stage 2 Clinical Quality Measure Data Elements at the Massachusetts eHealth Collaborative. 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
