

Cost-effectiveness of a European ST-segment elevation myocardial infarction network: results from the Catalan Codi Infart network
- PMID: 26656019
- PMCID: PMC4679883
- DOI: 10.1136/bmjopen-2015-009148
Cost-effectiveness of a European ST-segment elevation myocardial infarction network: results from the Catalan Codi Infart network
Abstract
Objectives: To evaluate the cost-effectiveness of the ST-segment elevation myocardial infarction (STEMI) network of Catalonia (Codi Infart).
Design: Cost-utility analysis.
Setting: The analysis was from the Catalonian Autonomous Community in Spain, with a population of about 7.5 million people.
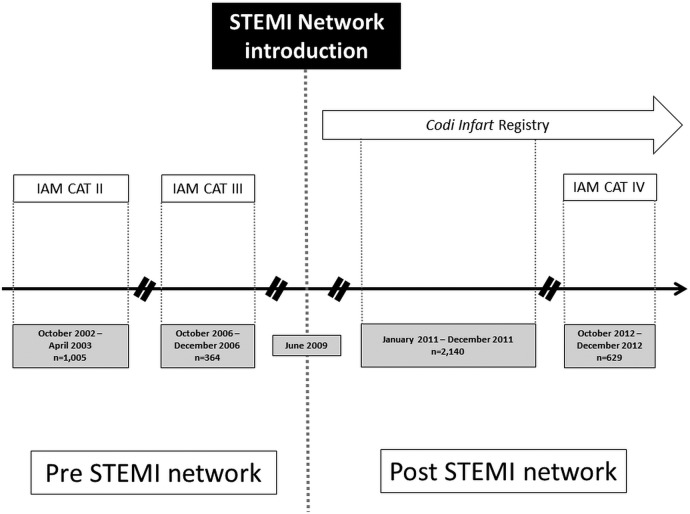
Participants: Patients with STEMI treated within the autonomous community of Catalonia (Spain) included in the IAM CAT II-IV and Codi Infart registries.
Outcome measures: Costs included hospitalisation, procedures and additional personnel and were obtained according to the reperfusion strategy. Clinical outcomes were defined as 30-day avoided mortality and quality-adjusted life-years (QALYs), before (N=356) and after network implementation (N=2140).
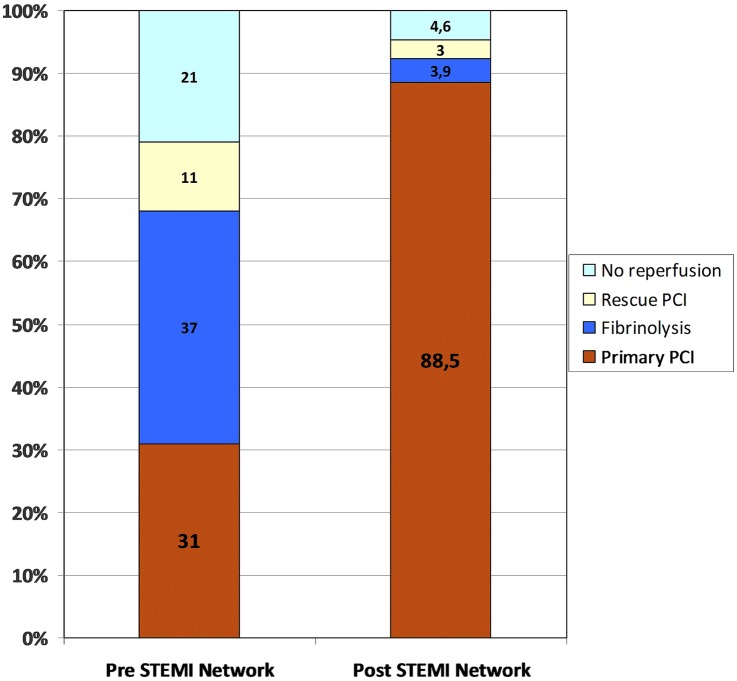
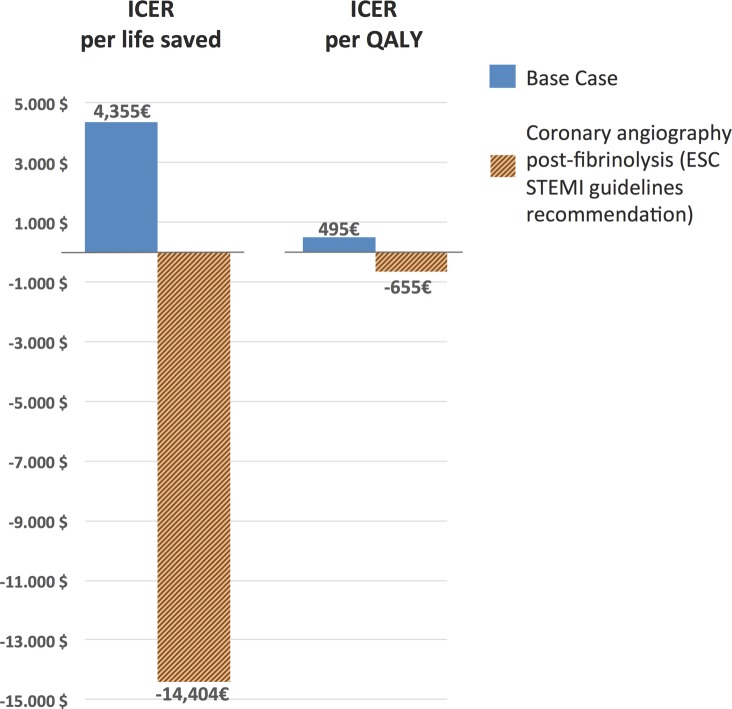
Results: A substitution effect and a technology effect were observed; aggregate costs increased by 2.6%. The substitution effect resulted from increased use of primary coronary angioplasty, a relatively expensive procedure and a decrease in fibrinolysis. Primary coronary angioplasty increased from 31% to 89% with the network, and fibrinolysis decreased from 37% to 3%. Rescue coronary angioplasty declined from 11% to 4%, and no reperfusion from 21% to 4%. The technological effect was related to improvements in the percutaneous coronary intervention procedure that increased efficiency, reducing the average length of the hospital stay. Mean costs per patient decreased from €8306 to €7874 for patients with primary coronary angioplasty. Clinical outcomes in patients treated with primary coronary angioplasty did not change significantly, although 30-day mortality decreased from 7.5% to 5.6%. The incremental cost-effectiveness ratio resulted in an extra cost of €4355 per life saved (30-day mortality) and €495 per QALY. Below a cost threshold of €30,000, results were sensitive to variations in costs and outcomes.
Conclusions: The Catalan STEMI network (Codi Infart) is cost-efficient. Further studies are needed in geopolitical different scenarios.
Keywords: HEALTH ECONOMICS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Steg PG, James SK, Atar D et al. , Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC)1. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012;33:2569–619. 10.1093/eurheartj/ehs215 - DOI - PubMed
-
- Widimský P, Groch L, Zelízko M et al. Multicentre randomized trial comparing transport to primary angioplasty vs immediate thrombolysis vs combined strategy for patients with acute myocardial infarction presenting to a community hospital without a catheterization laboratory. The PRAGUE study Eur Heart J 2000;21:823–31. 10.1053/euhj.1999.1993 - DOI - PubMed
-
- Khot UN, Johnson ML, Ramsey C et al. Emergency department physician activation of the catheterization laboratory and immediate transfer to an immediately available catheterization laboratory reduce door-to-balloon time in ST-elevation myocardial infarction. Circulation 2007;116:67–76. 10.1161/CIRCULATIONAHA.106.677401 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous