

Safety and Proof-of-Concept Study of Oral QLT091001 in Retinitis Pigmentosa Due to Inherited Deficiencies of Retinal Pigment Epithelial 65 Protein (RPE65) or Lecithin:Retinol Acyltransferase (LRAT)
- PMID: 26656277
- PMCID: PMC4687523
- DOI: 10.1371/journal.pone.0143846
Safety and Proof-of-Concept Study of Oral QLT091001 in Retinitis Pigmentosa Due to Inherited Deficiencies of Retinal Pigment Epithelial 65 Protein (RPE65) or Lecithin:Retinol Acyltransferase (LRAT)
Abstract
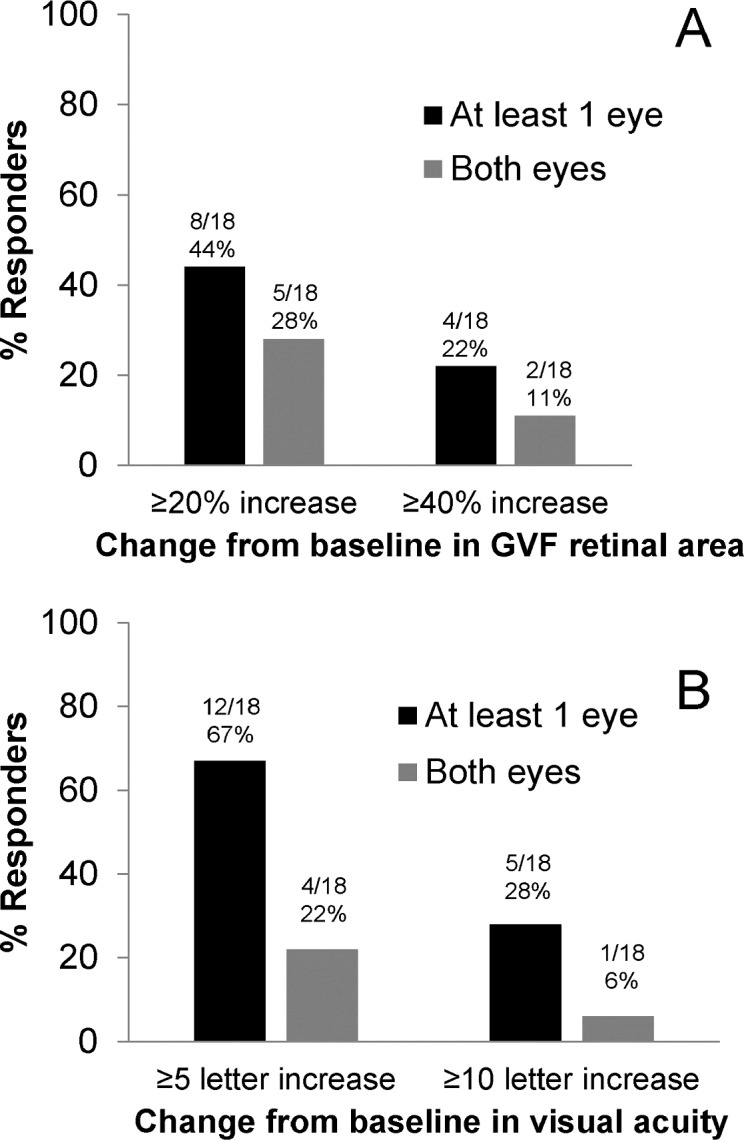
Restoring vision in inherited retinal degenerations remains an unmet medical need. In mice exhibiting a genetically engineered block of the visual cycle, vision was recently successfully restored by oral administration of 9-cis-retinyl acetate (QLT091001). Safety and visual outcomes of a once-daily oral dose of 40 mg/m2/day QLT091001 for 7 consecutive days was investigated in an international, multi-center, open-label, proof-of-concept study in 18 patients with RPE65- or LRAT-related retinitis pigmentosa. Eight of 18 patients (44%) showed a ≥20% increase and 4 of 18 (22%) showed a ≥40% increase in functional retinal area determined from Goldmann visual fields; 12 (67%) and 5 (28%) of 18 patients showed a ≥5 and ≥10 ETDRS letter score increase of visual acuity, respectively, in one or both eyes at two or more visits within 2 months of treatment. In two patients who underwent fMRI, a significant positive response was measured to stimuli of medium contrast, moving, pattern targets in both left and right hemispheres of the occipital cortex. There were no serious adverse events. Treatment-related adverse events were transient and the most common included headache, photophobia, nausea, vomiting, and minor biochemical abnormalities. Measuring the outer segment length of the photoreceptor layer with high-definition optical coherence tomography was highly predictive of treatment responses with responders having a significantly larger baseline outer segment thickness (11.7 ± 4.8 μm, mean ± 95% CI) than non-responders (3.5 ± 1.2 μm). This structure-function relationship suggests that treatment with QLT091001 is more likely to be efficacious if there is sufficient photoreceptor integrity.
Trial registration: ClinicalTrials.gov NCT01014052.
Conflict of interest statement
Figures



Similar articles
-
Oral 9-cis retinoid for childhood blindness due to Leber congenital amaurosis caused by RPE65 or LRAT mutations: an open-label phase 1b trial.Lancet. 2014 Oct 25;384(9953):1513-20. doi: 10.1016/S0140-6736(14)60153-7. Epub 2014 Jul 13. Lancet. 2014. PMID: 25030840 Clinical Trial.
-
Outer Segment Thickness Predicts Visual Field Response to QLT091001 in Patients with RPE65 or LRAT Mutations.Transl Vis Sci Technol. 2015 Oct 1;4(5):8. doi: 10.1167/tvst.4.5.8. eCollection 2015 Oct. Transl Vis Sci Technol. 2015. PMID: 26448901 Free PMC article.
-
Vitamin A derivatives as treatment options for retinal degenerative diseases.Nutrients. 2013 Jul 12;5(7):2646-66. doi: 10.3390/nu5072646. Nutrients. 2013. PMID: 23857173 Free PMC article. Review.
-
Loss of cone photoreceptors caused by chromophore depletion is partially prevented by the artificial chromophore pro-drug, 9-cis-retinyl acetate.Hum Mol Genet. 2009 Jun 15;18(12):2277-87. doi: 10.1093/hmg/ddp163. Epub 2009 Apr 1. Hum Mol Genet. 2009. PMID: 19339306 Free PMC article.
-
Pharmacotherapy of retinal disease with visual cycle modulators.Expert Opin Pharmacother. 2018 Apr;19(5):471-481. doi: 10.1080/14656566.2018.1448060. Epub 2018 Mar 15. Expert Opin Pharmacother. 2018. PMID: 29542350 Review.
Cited by
-
Fundus Albipunctatus Associated with Biallelic LRAT Gene Mutation: A Case Report with Long-Term Follow-Up.J Clin Med. 2023 Nov 7;12(22):6960. doi: 10.3390/jcm12226960. J Clin Med. 2023. PMID: 38002575 Free PMC article.
-
The Role of Vitamin A in Retinal Diseases.Int J Mol Sci. 2022 Jan 18;23(3):1014. doi: 10.3390/ijms23031014. Int J Mol Sci. 2022. PMID: 35162940 Free PMC article. Review.
-
Enhancing Understanding of the Visual Cycle by Applying CRISPR/Cas9 Gene Editing in Zebrafish.Front Cell Dev Biol. 2018 Apr 11;6:37. doi: 10.3389/fcell.2018.00037. eCollection 2018. Front Cell Dev Biol. 2018. PMID: 29696141 Free PMC article. Review.
-
Lecithin:Retinol Acyltransferase: A Key Enzyme Involved in the Retinoid (visual) Cycle.Biochemistry. 2016 Jun 7;55(22):3082-91. doi: 10.1021/acs.biochem.6b00319. Epub 2016 May 23. Biochemistry. 2016. PMID: 27183166 Free PMC article. Review.
-
Unraveling the mysteries of pre-mRNA splicing in the retina via stem cell technology.Stem Cell Investig. 2016 Nov 4;3:72. doi: 10.21037/sci.2016.10.05. eCollection 2016. Stem Cell Investig. 2016. PMID: 27868054 Free PMC article. No abstract available.
References
-
- Berger W, Kloeckener-Gruissem B, Neidhardt J. The molecular basis of human retinal and vitreoretinal diseases. Prog Ret Eye Res. 2010;29:335–375. - PubMed
-
- Finger RP, Fimmers R, Holz FG, Scholl HP. Prevalence and causes of registered blindness in the largest federal state of Germany. Brit J Ophthalmol. 2011;95:1061–1067. - PubMed
-
- Rattner A, Sun H, Nathans J. Molecular genetics of human retinal disease. Annu Rev Genet. 1999;33:89–131. - PubMed
-
- Haim M. Epidemiology of retinitis pigmentosa in Denmark. Acta Ophthalmol Scand Suppl. 2002;80:1–34. - PubMed
-
- Hartong DT, Berson EL, Dryja TP. Retinitis pigmentosa. Lancet. 2006;368:1795–1809. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
