

Complete Remission in the Nephrotic Syndrome Study Network
- PMID: 26656320
- PMCID: PMC4702222
- DOI: 10.2215/CJN.02560315
Complete Remission in the Nephrotic Syndrome Study Network
Abstract
Background and objectives: This analysis from the Nephrotic Syndrome Study Network (NEPTUNE) assessed the phenotypic and pathology characteristics of proteinuric patients undergoing kidney biopsy and defined the frequency and factors associated with complete proteinuria remission (CRever).
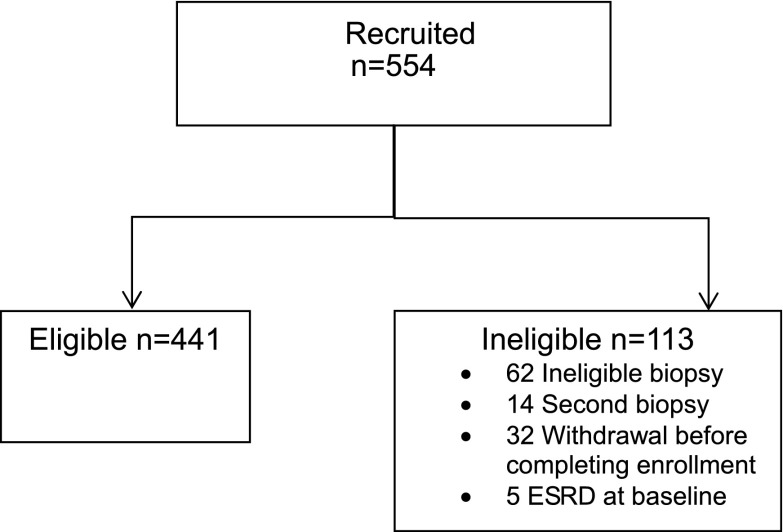
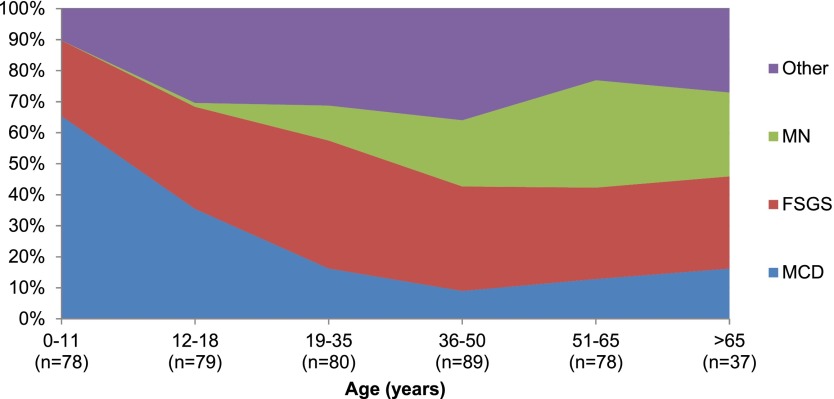
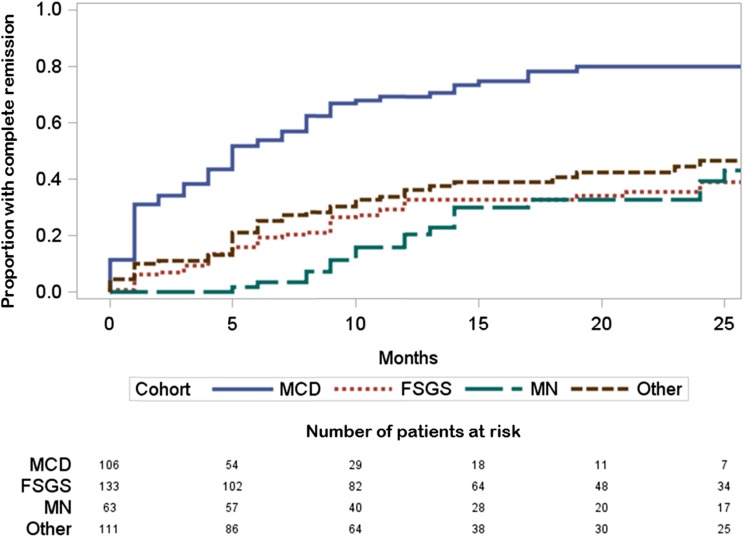
Design, setting, participants, & measurements: We enrolled adults and children with proteinuria ≥0.5 g/d at the time of first clinically indicated renal biopsy at 21 sites in North America from April 2010 to June 2014 into a prospective cohort study. NEPTUNE central pathologists assigned participants to minimal-change disease (MCD), FSGS, membranous nephropathy, or other glomerulopathy cohorts. Outcome measures for this analysis were (1) CRever with urine protein-to-creatinine ratio (UPC) <0.3 g/g with preserved native kidney function and (2) ESRD. Continuous variables are reported as median and interquartile range (IQR; 25th, 75th percentile). Cox proportional hazards modeling was used to assess factors associated with CRever.
Results: We enrolled 441 patients: 116 (27%) had MCD, 142 (32%) had FSGS, 66 (15%) had membranous nephropathy, and 117 (27%) had other glomerulopathy. The baseline UPC was 4.1 g/g (IQR, 1.9, 7.7) and the eGFR was 81 ml/min per 1.73 m(2) (IQR, 50, 105). Median duration of observation was 19 months (IQR, 11, 30). CRever occurred in 46% of patients, and 4.6% progressed to ESRD. Multivariate analysis demonstrated that higher prebiopsy proteinuria (hazard ratio, 0.3; 95% confidence interval, 0.2 to 0.5) and pathology diagnosis (FSGS versus MCD; hazard ratio, 0.2; 95% confidence interval, 0.1 to 0.5) were inversely associated with CRever. The effect of immunosuppressive therapy on remission varied by pathology diagnosis.
Conclusions: In NEPTUNE, the high frequency of other pathology in proteinuric patients affirms the value of the diagnostic kidney biopsy. Clinical factors, including level of proteinuria before biopsy, pathology diagnosis, and immunosuppression, are associated with complete remission.
Keywords: cohort studies; focal segmental glomerulosclerosis; glomerular filtration rate; humans; kidney biopsy; kidney failure chronic, proteinuria; membranous nephropathy; minimal change disease; nephrotic syndrome.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- US Renal Data System: USRDS 2014 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, 2014
-
- Gadegbeku CA, Gipson DS, Holzman LB, Ojo AO, Song PX, Barisoni L, Sampson MG, Kopp JB, Lemley KV, Nelson PJ, Lienczewski CC, Adler SG, Appel GB, Cattran DC, Choi MJ, Contreras G, Dell KM, Fervenza FC, Gibson KL, Greenbaum LA, Hernandez JD, Hewitt SM, Hingorani SR, Hladunewich M, Hogan MC, Hogan SL, Kaskel FJ, Lieske JC, Meyers KE, Nachman PH, Nast CC, Neu AM, Reich HN, Sedor JR, Sethna CB, Trachtman H, Tuttle KR, Zhdanova O, Zilleruelo GE, Kretzler M: Design of the Nephrotic Syndrome Study Network (NEPTUNE) to evaluate primary glomerular nephropathy by a multidisciplinary approach. Kidney Int 83: 749–756, 2013 - PMC - PubMed
-
- Barisoni L, Nast CC, Jennette JC, Hodgin JB, Herzenberg AM, Lemley KV, Conway CM, Kopp JB, Kretzler M, Lienczewski C, Avila-Casado C, Bagnasco S, Sethi S, Tomaszewski J, Gasim AH, Hewitt SM: Digital pathology evaluation in the multicenter Nephrotic Syndrome Study Network (NEPTUNE). Clin J Am Soc Nephrol 8: 1449–1459, 2013 - PMC - PubMed
-
- Friedewald WT, Levy RI, Fredrickson DS: Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18: 499–502, 1972 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
