

Comparison of National Operative Mortality in Gastroenterological Surgery Using Web-based Prospective Data Entry Systems
- PMID: 26656350
- PMCID: PMC5008495
- DOI: 10.1097/MD.0000000000002194
Comparison of National Operative Mortality in Gastroenterological Surgery Using Web-based Prospective Data Entry Systems
Abstract
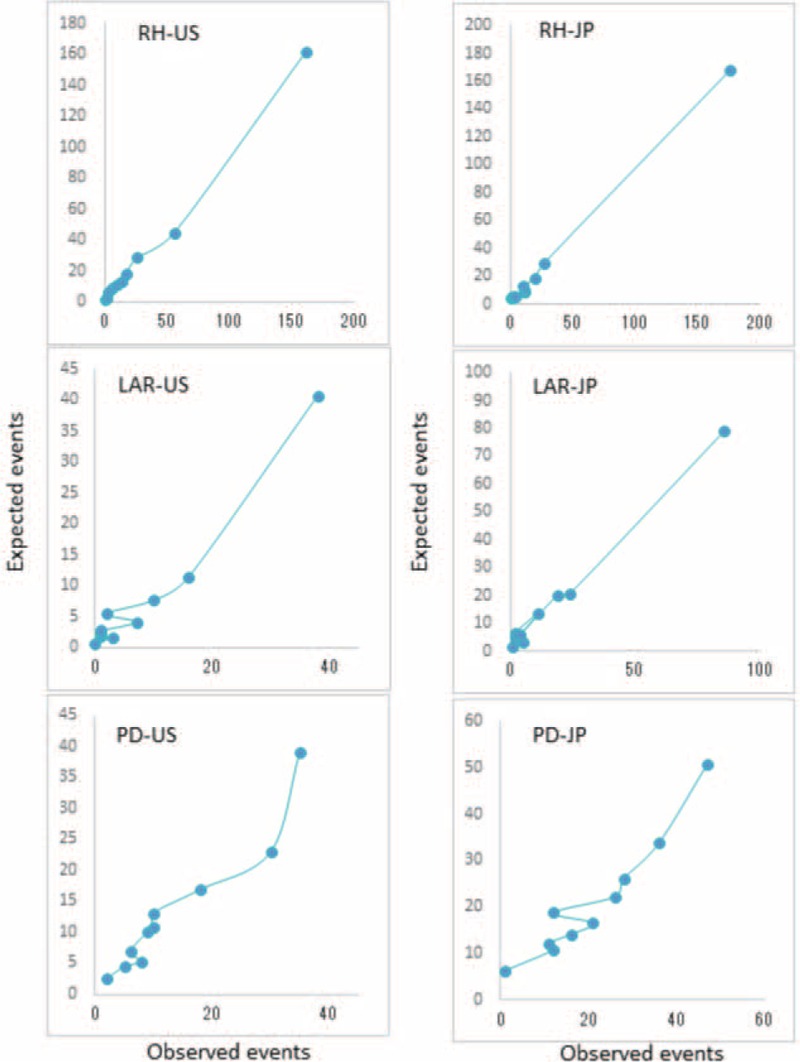
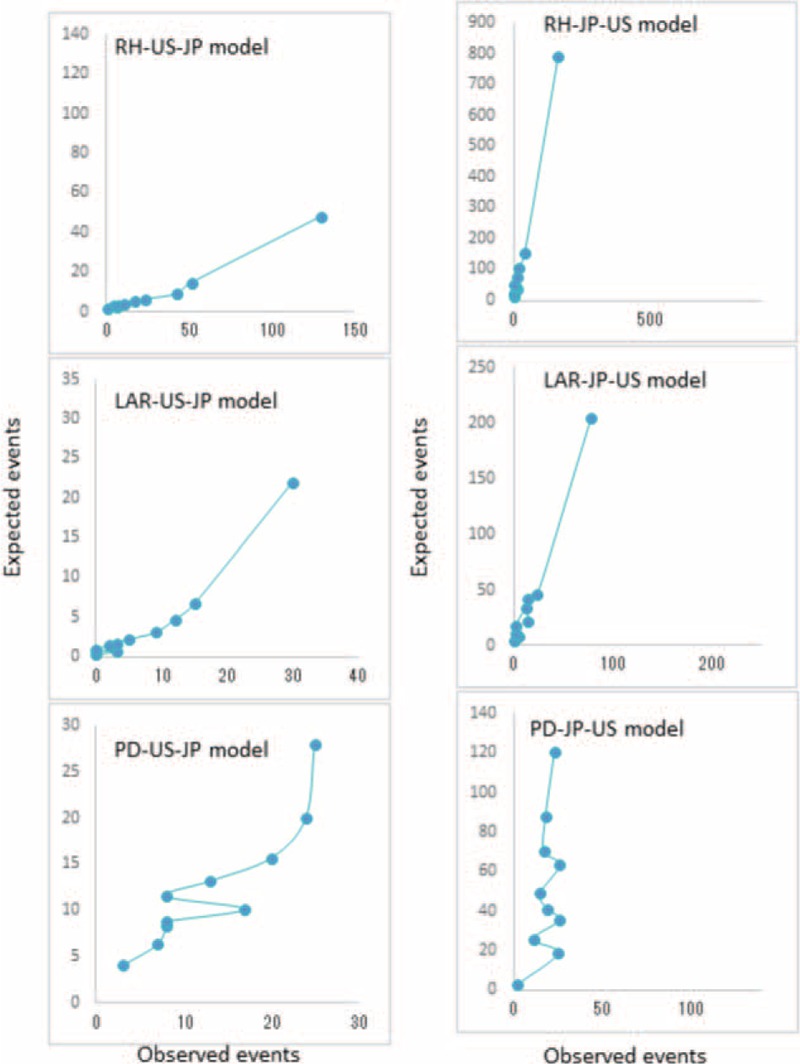
International collaboration is important in healthcare quality evaluation; however, few international comparisons of general surgery outcomes have been accomplished. Furthermore, predictive model application for risk stratification has not been internationally evaluated. The National Clinical Database (NCD) in Japan was developed in collaboration with the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP), with a goal of creating a standardized surgery database for quality improvement. The study aimed to compare the consistency and impact of risk factors of 3 major gastroenterological surgical procedures in Japan and the United States (US) using web-based prospective data entry systems: right hemicolectomy (RH), low anterior resection (LAR), and pancreaticoduodenectomy (PD).Data from NCD and ACS-NSQIP, collected over 2 years, were examined. Logistic regression models were used for predicting 30-day mortality for both countries. Models were exchanged and evaluated to determine whether the models built for one population were accurate for the other population.We obtained data for 113,980 patients; 50,501 (Japan: 34,638; US: 15,863), 42,770 (Japan: 35,445; US: 7325), and 20,709 (Japan: 15,527; US: 5182) underwent RH, LAR, and, PD, respectively. Thirty-day mortality rates for RH were 0.76% (Japan) and 1.88% (US); rates for LAR were 0.43% versus 1.08%; and rates for PD were 1.35% versus 2.57%. Patient background, comorbidities, and practice style were different between Japan and the US. In the models, the odds ratio for each variable was similar between NCD and ACS-NSQIP. Local risk models could predict mortality using local data, but could not accurately predict mortality using data from other countries.We demonstrated the feasibility and efficacy of the international collaborative research between Japan and the US, but found that local risk models remain essential for quality improvement.
Conflict of interest statement
disclosures: The authors report no conflicting financial interests.
Figures
References
-
- Hall BL, Hamilton BH, Richards K, et al. Does surgical quality improve in the American College of Surgeons National Surgical Quality Improvement Program: an evaluation of all participating hospitals. Ann Surg 2009; 250:363–376. - PubMed
-
- Miyata H, Gotoh M, Hashimoto H, et al. Challenges and prospects of a clinical database linked to the board certification system. Surg Today 2014; 44:1991–1999. - PubMed
-
- Anazawa T, Miyata H, Gotoh M. Cancer registries in Japan: National Clinical Database and site-specific cancer registries. Int J Clin Oncol 2015; 20:5–10. - PubMed
-
- Cohen ME, Ko CY, Bilimoria KY, et al. Optimizing ACS NSQIP modeling for evaluation of surgical quality and risk: patient risk adjustment, procedure mix adjustment, shrinkage adjustment, and surgical focus. J Am Coll Surg 2013; 217:336–346. - PubMed
-
- Khuri SF, Henderson WG, Daley J, et al. Successful implementation of the Department of Veterans Affairs’ National Surgical Quality Improvement Program in the private sector: the Patient Safety in Surgery study. Ann Surg 2008; 248:329–336. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
