

The Value of U/S to Determine Priority for Upper Gastrointestinal Endoscopy in Emergency Room
- PMID: 26656368
- PMCID: PMC5008513
- DOI: 10.1097/MD.0000000000002241
The Value of U/S to Determine Priority for Upper Gastrointestinal Endoscopy in Emergency Room
Erratum in
- Medicine (Baltimore). 2016 Jan;95(1):1
-
Erratum: The Value of U/S to Determine Priority for Upper Gastrointestinal Endoscopy in Emergency Room: Erratum.Medicine (Baltimore). 2016 Jan 8;95(1):e0688. doi: 10.1097/01.md.0000479433.86506.88. eCollection 2016 Jan. Medicine (Baltimore). 2016. PMID: 31265550 Free PMC article.
Abstract
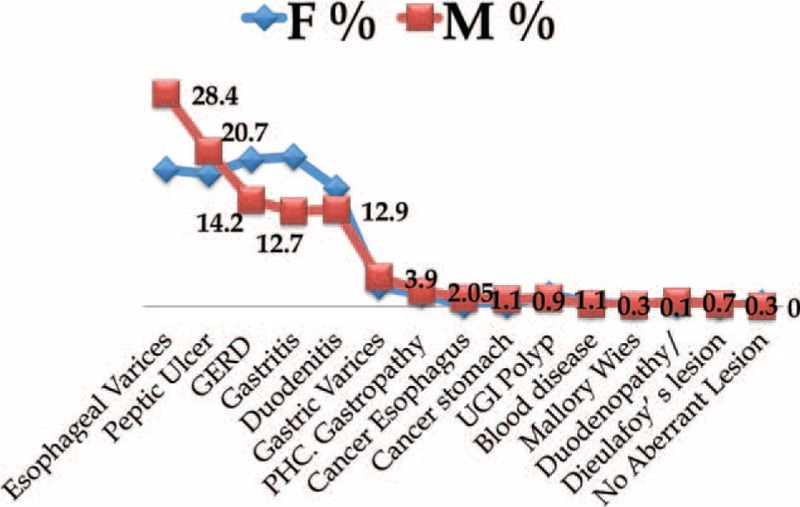
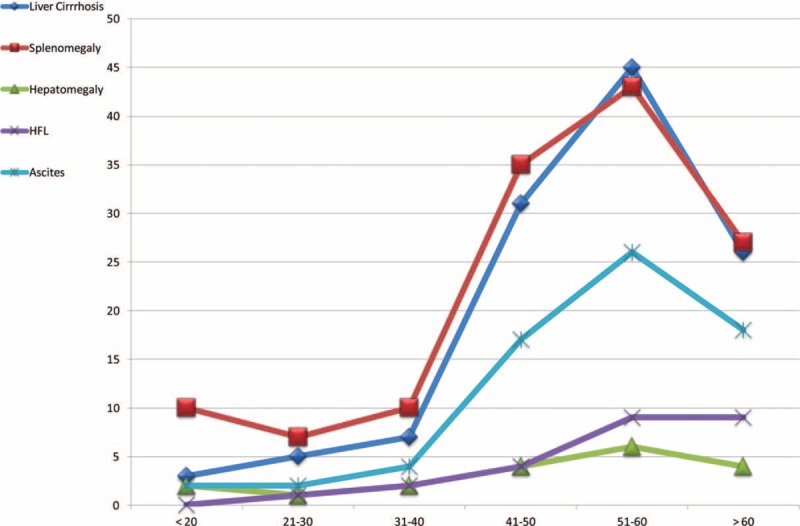
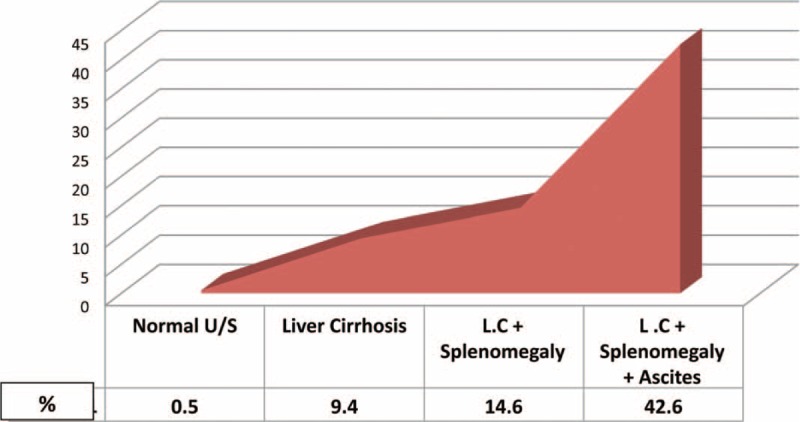
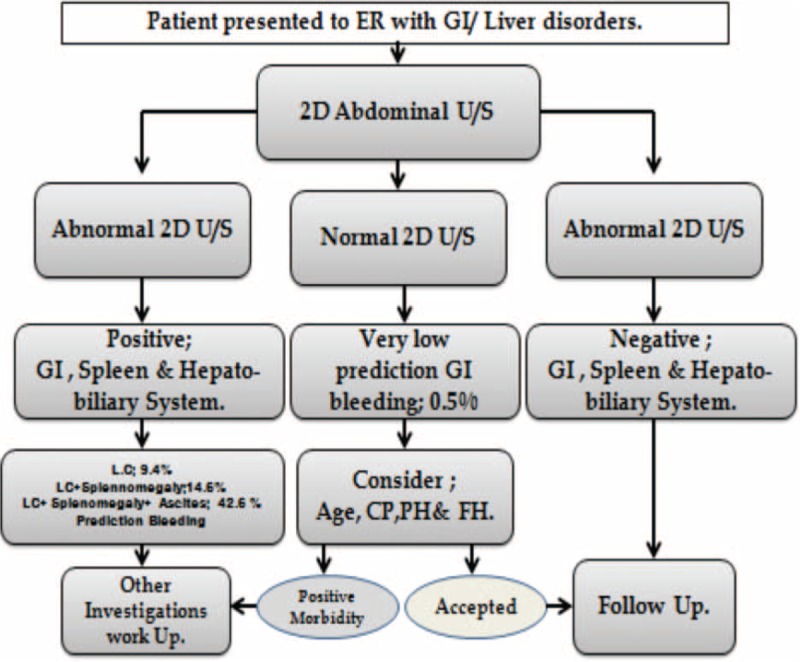
In countries endemic for liver and GIT diseases, frequent emergency department (ED) patients contribute to a disproportionate number of visits consuming substantial amount of medical resources. One of the most frequent ED visits is patients who present with hypovolemic shock, abdominal pain, or confusion with or without signs of upper gastrointestinal bleeding (UGIB). The use of conventional two-dimensional ultrasound (2D-U/S) may provide immediate and useful information on the presence of esophageal varices, gastrointestinal tumors, and other GIT abnormalities.The current study investigated the feasibility of using (2D-U/S) to predict the source of UGIB in ED and to determine patients' priority for UGE.Between February 2003 and March 2013, we retrospectively reviewed the profiles of 38,551 Egyptian patients, aged 2 to 75 years old, who presented with a history of GI/liver diseases and no alcohol consumption. We assessed the value of 2D-U/S technology in predicting the source of UGIB.Of 38,551 patients presenting to ED, 900 patients (2.3%), 534 male (59.3%) and 366 female (40.7%) developed UGIB. Analyzing results obtained from U/S examinations by data mining for emergent UGE were patients with liver cirrhosis (LC), splenomegaly, and ascites (42.6% incidence of UGIB), followed by LC and splenomegaly (14.6%), LC only (9.4%), and was only 0.5% who had no morbidity finding by 2D-U/S.Ultrasonographic instrumentation increases the feasibility of predictive emergency medicine. The area has recently not only gained a fresh impulse, but also a new set of complex problems that needs to be addressed in the emergency medicine setting according to each priority.
Conflict of interest statement
The authors confirm the following statements: The manuscript is a unique submission and is not being considered for publication by any other source in any medium. Further, the manuscript has not been published, in part or in full, in any form. That there has been no duplicate publication or submission elsewhere of any part of the work (excluding abstracts); That all authors have read and approved the report; and That there were no financial or other relations that could lead to a conflict of interest. The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Demographic profile and endoscopic findings among patients with upper gastrointestinal bleeding in Ahmadu Bello University Teaching Hospital, Zaria, North-Western Nigeria.Niger J Clin Pract. 2020 Aug;23(8):1163-1166. doi: 10.4103/njcp.njcp_69_20. Niger J Clin Pract. 2020. PMID: 32788496
-
Endoscopic findings in upper gastrointestinal bleeding patients at Lacor hospital, northern Uganda.Afr Health Sci. 2012 Dec;12(4):518-21. doi: 10.4314/ahs.v12i4.19. Afr Health Sci. 2012. PMID: 23515280 Free PMC article.
-
Causes of bleeding and outcomes in patients hospitalized with upper gastrointestinal bleeding.J Clin Gastroenterol. 2014 Feb;48(2):113-8. doi: 10.1097/MCG.0b013e318297fb40. J Clin Gastroenterol. 2014. PMID: 23685847
-
Age-specific causes of upper gastrointestinal bleeding in children.World J Gastroenterol. 2023 Dec 21;29(47):6095-6110. doi: 10.3748/wjg.v29.i47.6095. World J Gastroenterol. 2023. PMID: 38186684 Free PMC article. Review.
-
Upper and lower gastrointestinal bleeding in the elderly.Gastroenterol Clin North Am. 1990 Jun;19(2):293-318. Gastroenterol Clin North Am. 1990. PMID: 2194947 Review.
Cited by
-
Performance of Three Scoring Systems in Predicting Massive Transfusion in Patients with Unstable Upper Gastrointestinal Hemorrhage.Yonsei Med J. 2019 Apr;60(4):368-374. doi: 10.3349/ymj.2019.60.4.368. Yonsei Med J. 2019. PMID: 30900423 Free PMC article.
-
Causes of Melena and Effective Examination Strategies in Children.Front Pediatr. 2021 Dec 8;9:780356. doi: 10.3389/fped.2021.780356. eCollection 2021. Front Pediatr. 2021. PMID: 34956987 Free PMC article.
-
Incidence of HCV induced-Esophageal varices in Egypt: Valuable knowledge using data mining analysis.Medicine (Baltimore). 2017 Jan;96(4):e5647. doi: 10.1097/MD.0000000000005647. Medicine (Baltimore). 2017. PMID: 28121921 Free PMC article.
-
Erratum: The Value of U/S to Determine Priority for Upper Gastrointestinal Endoscopy in Emergency Room: Erratum.Medicine (Baltimore). 2016 Jan 8;95(1):e0688. doi: 10.1097/01.md.0000479433.86506.88. eCollection 2016 Jan. Medicine (Baltimore). 2016. PMID: 31265550 Free PMC article.
References
-
- Barkun AN, Bardou M, KuipersEJ, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med 2010; 152:101. - PubMed
-
- Balderas V, Bhore R, Lara LF, et al. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med 2011; 124:970–976. - PubMed
-
- Cappell MS, Friedel D. Initial management of acute upper gastrointestinal bleeding: from initial evaluation up to gastrointestinal endoscopy. Med Clin North Am 2008; 92:491. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
