

Factors Associated With Unplanned Hospitalizations Among Patients With Nonmetastatic Colorectal Cancers Intended for Treatment in the Ambulatory Setting
- PMID: 26657478
- PMCID: PMC4811187
- DOI: 10.1097/NNR.0000000000000134
Factors Associated With Unplanned Hospitalizations Among Patients With Nonmetastatic Colorectal Cancers Intended for Treatment in the Ambulatory Setting
Abstract
Background: Chemotherapy administration and supportive management for solid tumors is intended to take place in the ambulatory setting, but little is known about why some patients experience treatment-related adverse events so severe as to require acute inpatient care.
Objective: The aim of the study was to identify predictors of initial and repeated unplanned hospitalizations and potential financial impact among Medicare patients with early-stage (Stages I-III) colorectal cancer receiving outpatient chemotherapy.
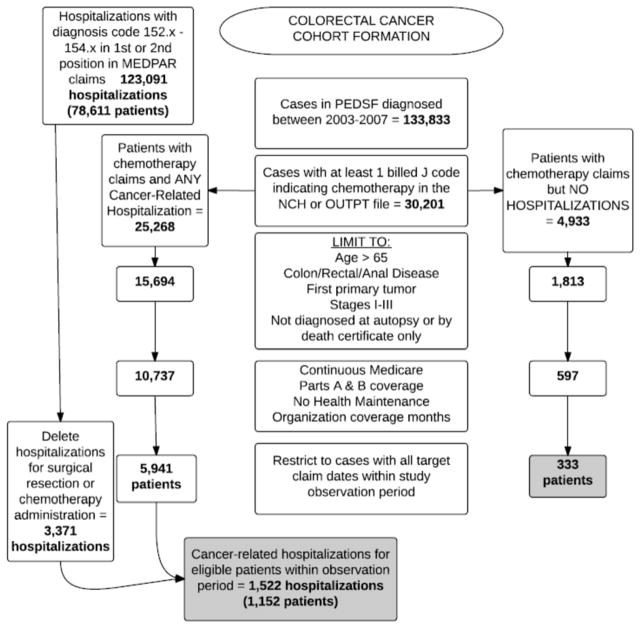
Methods: Advanced statistical modeling was used to analyze a cohort of patients (N = 1,485) from the Surveillance, Epidemiology, and End Results (SEER)-Medicare database diagnosed from 2003 to 2007 with colorectal cancer as their first primary malignancy. Patients were of ages 66 and older at diagnosis, had uninterrupted Medicare Parts A and B coverage with no health maintenance organization component, and received chemotherapy at least one time.
Results: Female gender, younger age, multiple comorbidities, rural geography, higher high school completion rates, and lower median income per census tract were significant predictors of the likelihood of initial unplanned hospitalizations. Non-White race, receipt of radiation therapy, rural geography, and higher weighted comorbidity scores were factors associated with the number of hospitalizations experienced. The total Medicare charges calculated for these admissions was $38,976,171, with the median charge per admission at $20,412.
Discussion: Demographic and clinical factors that form the foundation of work toward development of a risk factor profile for unplanned hospitalization were identified. Further work is needed to incorporate additional clinical data to create a clinically applicable model.
Conflict of interest statement
The authors report no conflicts of interest to report.
Figures
Similar articles
-
Predictors of Unplanned Hospitalizations in Patients With Nonmetastatic Lung Cancer During Chemotherapy.Oncol Nurs Forum. 2017 Sep 1;44(5):E203-E212. doi: 10.1188/17.ONF.E203-E212. Oncol Nurs Forum. 2017. PMID: 28820513 Free PMC article.
-
Trends in end-of-life care and health care spending in women with uterine cancer.Am J Obstet Gynecol. 2017 Oct;217(4):434.e1-434.e10. doi: 10.1016/j.ajog.2017.07.006. Epub 2017 Jul 11. Am J Obstet Gynecol. 2017. PMID: 28709581 Free PMC article.
-
A patient's race/ethnicity does not explain the underuse of appropriate adjuvant therapy in colorectal cancer.Dis Colon Rectum. 2006 Mar;49(3):319-29. doi: 10.1007/s10350-005-0283-6. Dis Colon Rectum. 2006. PMID: 16475031
-
Surgeon characteristics and receipt of adjuvant radiotherapy in women with breast cancer.J Natl Cancer Inst. 2008 Feb 6;100(3):199-206. doi: 10.1093/jnci/djm320. Epub 2008 Jan 29. J Natl Cancer Inst. 2008. PMID: 18230795
-
Patterns of Colorectal Cancer Care in the United States: 1990-2010.J Natl Cancer Inst. 2015 Jul 23;107(10):djv198. doi: 10.1093/jnci/djv198. Print 2015 Oct. J Natl Cancer Inst. 2015. PMID: 26206950 Free PMC article.
Cited by
-
Bayesian Network Analysis for Prediction of Unplanned Hospital Readmissions of Cancer Patients with Breakthrough Cancer Pain and Complex Care Needs.Healthcare (Basel). 2022 Sep 23;10(10):1853. doi: 10.3390/healthcare10101853. Healthcare (Basel). 2022. PMID: 36292299 Free PMC article.
-
Are we "missing the big picture" in transitions of care? Perspectives of healthcare providers managing patients with unplanned hospitalization.Appl Nurs Res. 2018 Dec;44:60-66. doi: 10.1016/j.apnr.2018.09.006. Epub 2018 Sep 19. Appl Nurs Res. 2018. PMID: 30389062 Free PMC article.
-
Influence of Education Level of Older Patients on Polypharmacy, Potentially Inappropriate Medications Listed in Beer's Criteria, and Unplanned Hospitalization: A Cross-Sectional Study in Lahore, Pakistan.Medicina (Kaunas). 2018 Aug 24;54(4):57. doi: 10.3390/medicina54040057. Medicina (Kaunas). 2018. PMID: 30344288 Free PMC article.
-
Assessment of prescribing potentially inappropriate medications listed in Beers criteria and its association with the unplanned hospitalization: a cross-sectional study in Lahore, Pakistan.Clin Interv Aging. 2018 Aug 28;13:1485-1495. doi: 10.2147/CIA.S173942. eCollection 2018. Clin Interv Aging. 2018. PMID: 30214169 Free PMC article.
-
The Impact of Intensity Modulated Radiation Therapy on Hospitalization Outcomes in the SEER-Medicare Population With Anal Squamous Cell Carcinoma.Int J Radiat Oncol Biol Phys. 2017 May 1;98(1):177-185. doi: 10.1016/j.ijrobp.2017.01.006. Epub 2017 Jan 7. Int J Radiat Oncol Biol Phys. 2017. PMID: 28258896 Free PMC article.
References
-
- Aparicio T, Jouve JL, Teillet L, Gargot D, Subtil F, Le Brun-Ly V, … Mitry E. Geriatric factors predict chemotherapy feasibility: Ancillary results of FFCD 2001–02 phase III study in first-line chemotherapy for metastatic colorectal cancer in elderly patients. Journal of Clinical Oncology. 2013;31:1464–1470. doi: 10.1200/JCO.2012.42.9894. - DOI - PubMed
-
- Baglan KL, Frazier RC, Yan D, Huang RR, Martinez AA, Robertson JM. The dose-volume realationship of acute small bowel toxicity from concurrent 5-FU-based chemotherapy and radiation therapy for rectal cancer. International Journal of Radiation Oncology Biology•Physics. 2002;52:176–183. doi: 10.1016/S0360-3016(01)01820-X. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
