

Surveillance of IBD Using High Definition Colonoscopes Does Not Miss Adenocarcinoma in Patients with Low-grade Dysplasia
- PMID: 26658214
- PMCID: PMC5058785
- DOI: 10.1097/MIB.0000000000000634
Surveillance of IBD Using High Definition Colonoscopes Does Not Miss Adenocarcinoma in Patients with Low-grade Dysplasia
Abstract
Background: Historically, limits to the ability to detect dysplasia in chronic inflammatory bowel disease (IBD)-associated colitis resulted in the recommendation that neoplasia of any grade be treated by proctocolectomy. We hypothesized that with improved optical technologies, most neoplasia in colitis is now detectable and reassessed the prevalence of colitis-associated neoplasia.
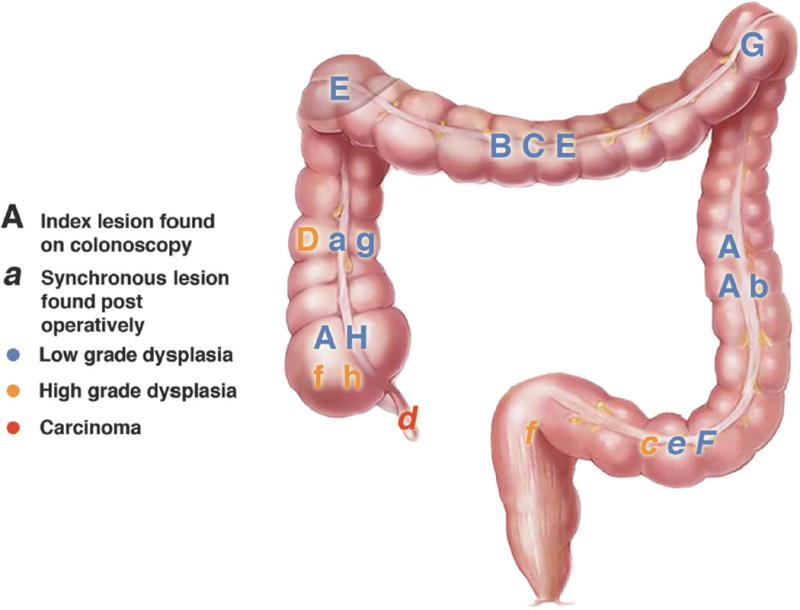
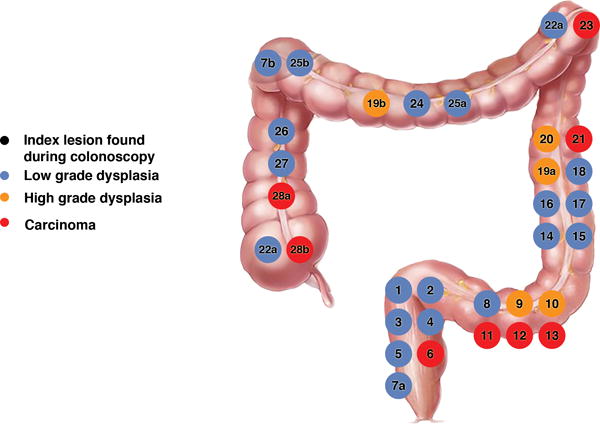
Methods: We retrospectively reviewed all our patients with IBD who had pathologist-confirmed neoplasia on surveillance colonoscopy and underwent a subsequent colectomy. We included patients whose index lesions were found between 2005 and 2014 (the dates of our high definition equipment) and recorded the location and grade of these lesions. These findings were compared to the surgical specimens, and in patients with partial colectomies, included follow-up.
Results: Thirty-six patients with IBD (19 [53%] ulcerative colitis and 17 [47%] Crohn's disease) were found to have neoplastic lesions on surveillance colonoscopy and underwent a subsequent partial colectomy or total proctocolectomy. Forty-four index lesions were identified by colonoscopy (29 white light and 7 methylene blue chromoscopy): 30 low-grade dysplasia, 6 high-grade dysplasia, and 8 adenocarcinoma. None of the low-grade dysplasia or adenocarcinoma index lesions were associated with synchronous carcinoma at colectomy. One of the patients with high-grade dysplasia had adenocarcinoma of the appendix.
Conclusions: In this experience with high definition colonoscopes in chronic colitis, no synchronous adenocarcinomas were found when colectomy was performed for low-grade dysplasia or index adenocarcinoma, and only 1 adenocarcinoma in the appendix was found in the setting of high-grade dysplasia. These findings suggest that active surveillance or subtotal colectomy may be safe options for patients with IBD and some grades of neoplasia.
Conflict of interest statement
The authors have no relevant conflicts of interest.
Figures
References
-
- Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory bowel disease. N Engl J Med. 2015;372:1441–52. - PubMed
-
- Ullman T, C V, Harpaz N, et al. Progression of flat low-grade dysplasia to advanced neoplasia in patients with ulcerative colitis. Gastroenterology. 2003;125:1311–9. - PubMed
-
- Soetikno RM, Lin OS, Heidenreich PA, et al. Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and ulcerative colitis: a meta-analysis. Gastrointest Endosc. 2002;56:48–54. - PubMed
-
- Rutter M, Saunders B, Wilkinson K, et al. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology. 2004;126:451–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
