

Effect of alteplase on the CT hyperdense artery sign and outcome after ischemic stroke
- PMID: 26658907
- PMCID: PMC4731690
- DOI: 10.1212/WNL.0000000000002236
Effect of alteplase on the CT hyperdense artery sign and outcome after ischemic stroke
Abstract
Objective: To investigate whether the location and extent of the CT hyperdense artery sign (HAS) at presentation affects response to IV alteplase in the randomized controlled Third International Stroke Trial (IST-3).
Methods: All prerandomization and follow-up (24-48 hours) CT brain scans in IST-3 were assessed for HAS presence, location, and extent by masked raters. We assessed whether HAS grew, persisted, shrank, or disappeared at follow-up, the association with 6-month functional outcome, and effect of alteplase. IST-3 is registered (ISRCTN25765518).
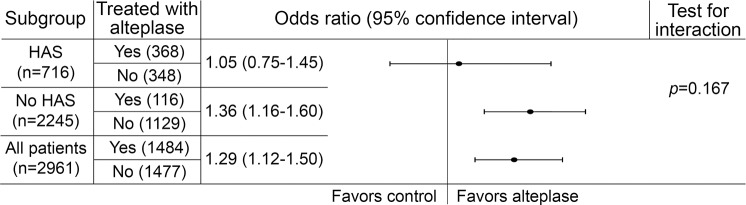
Results: HAS presence (vs absence) independently predicted poor 6-month outcome (increased Oxford Handicap Scale [OHS]) on adjusted ordinal regression analysis (odds ratio [OR] 0.66, p < 0.001). Outcome was worse in patients with more (vs less) extensive HAS (OR 0.61, p = 0.027) but not in proximal (vs distal) HAS (p = 0.420). Increasing age was associated with more HAS growth at follow-up (OR 1.01, p = 0.013). Treatment with alteplase increased HAS shrinkage/disappearance at follow-up (OR 0.77, p = 0.006). There was no significant difference in HAS shrinkage with alteplase in proximal (vs distal) or more (vs less) extensive HAS (p = 0.516 and p = 0.580, respectively). There was no interaction between presence vs absence of HAS and benefit of alteplase on 6-month OHS (p = 0.167).
Conclusions: IV alteplase promotes measurable reduction in HAS regardless of HAS location or extent. Alteplase increased independence at 6 months in patients with and without HAS.
Classification of evidence: This study provides Class I evidence that for patients within 6 hours of ischemic stroke with a CT hyperdense artery sign, IV alteplase reduced intra-arterial hyperdense thrombus.
© 2015 American Academy of Neurology.
Figures

References
-
- Wardlaw JM, Farrall AJ, Perry D, et al. Factors influencing the detection of early computed tomography signs of cerebral ischemia: an Internet-based, international multiobserver study. Stroke 2007;38:1250–1256. - PubMed
-
- Kharitonova T, Ahmed N, Thorén M, et al. Hyperdense middle cerebral artery sign on admission CT scan: prognostic significance for ischaemic stroke patients treated with intravenous thrombolysis in the safe implementation of thrombolysis in Stroke International Stroke Thrombolysis Register. Cerebrovasc Dis 2009;27:51–59. - PubMed
-
- Manelfe C, Larrue V, von Kummer R, et al. Association of hyperdense middle cerebral artery sign with clinical outcome in patients treated with tissue plasminogen activator. Stroke 1999;30:769–772. - PubMed
-
- Novotna J, Kadlecova P, Czlonkowska A, et al. Hyperdense cerebral artery computed tomography sign is associated with stroke severity rather than stroke subtype. J Stroke Cerebrovasc Dis 2014;23:2533–2539. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials