

Spatial Variation and Resuscitation Process Affecting Survival after Out-of-Hospital Cardiac Arrests (OHCA)
- PMID: 26659851
- PMCID: PMC4682793
- DOI: 10.1371/journal.pone.0144882
Spatial Variation and Resuscitation Process Affecting Survival after Out-of-Hospital Cardiac Arrests (OHCA)
Abstract
Background: Ambulance response times and resuscitation efforts are critical predictors of the survival rate after out-of-hospital cardiac arrests (OHCA). On the other hand, rural-urban differences in the OHCA survival rates are an important public health issue.
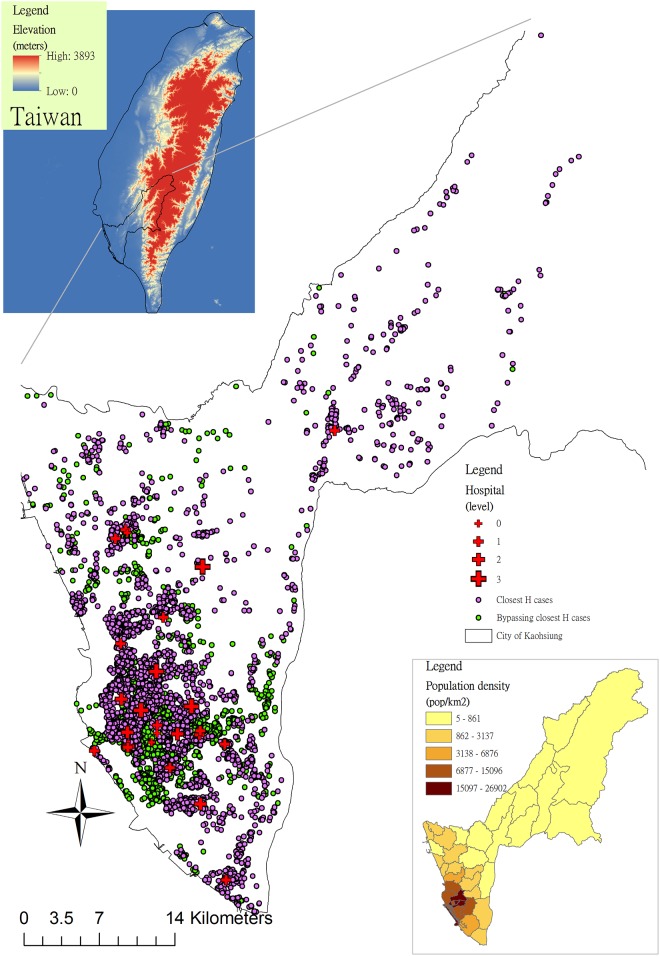
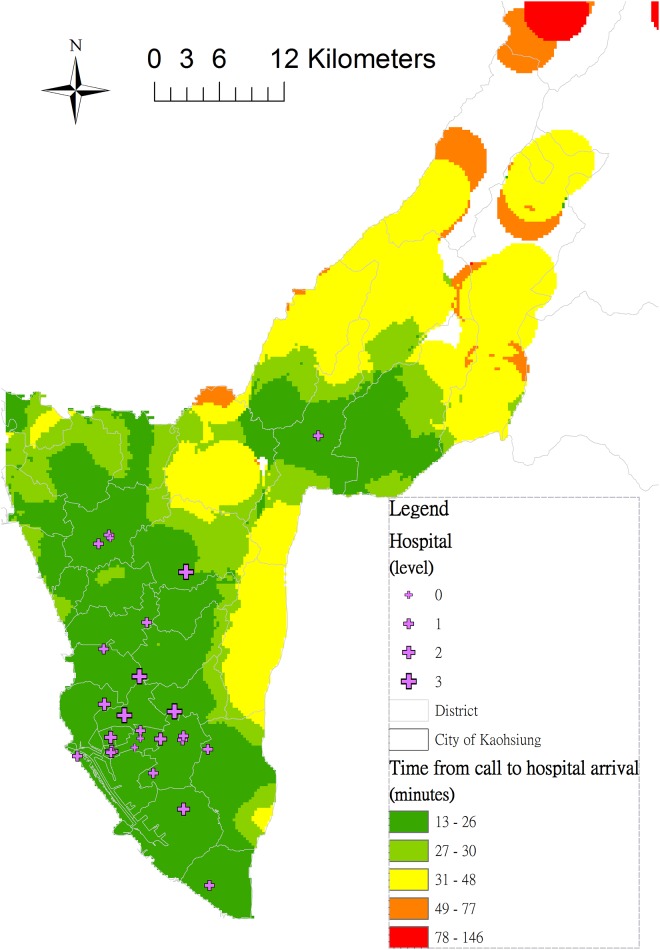
Methods: We retrospectively reviewed the January 2011-December 2013 OHCA registry data of Kaohsiung City, Taiwan. With particular focus on geospatial variables, we aimed to unveil risk factors predicting the overall OHCA survival until hospital admission. Spatial analysis, network analysis, and the Kriging method by using geographic information systems were applied to analyze spatial variations and calculate the transport distance. Logistic regression was used to identify the risk factors for OHCA survival.
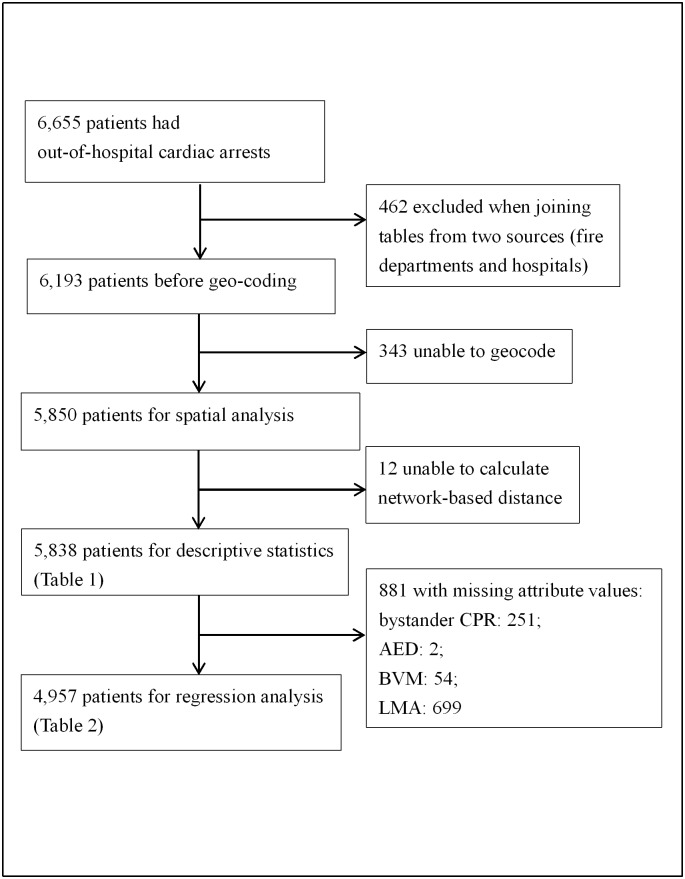
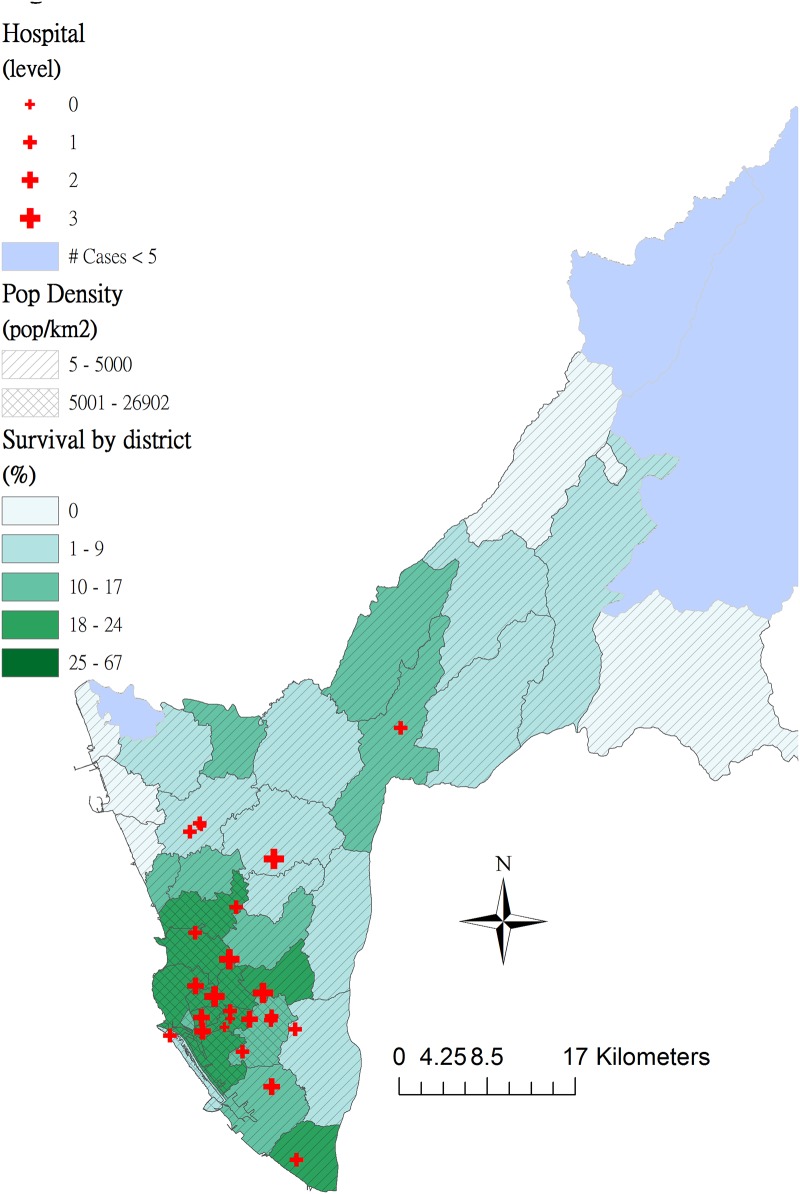
Results: Among the 4,957 patients, the overall OHCA survival to hospital admission was 16.5%. In the multivariate analysis, female sex (adjusted odds ratio:, AOR, 1.24 [1.06-1.45]), events in public areas (AOR: 1.30 [1.05-1.61]), exposure to automated external defibrillator (AED) shock (AOR: 1.70 [1.30-2.23]), use of laryngeal mask airway (LMA) (AOR: 1.35 [1.16-1.58]), non-trauma patients (AOR: 1.41 [1.04-1.90]), ambulance bypassed the closest hospital (AOR: 1.28 [1.07-1.53]), and OHCA within the high population density areas (AOR: 1.89 [1.55-2.32]) were positively associated with improved OHCA survival. By contrast, a prolonged total emergency medical services (EMS) time interval was negatively associated with OHCA survival (AOR: 0.98 [0.96-0.99]).
Conclusions: Resuscitative efforts, such as AED or LMA use, and a short total EMS time interval improved OHCA outcomes in emergency departments. The spatial heterogeneity of emergency medical resources between rural and urban areas might affect survival rate.
Conflict of interest statement
Figures
Similar articles
-
Out-of-hospital cardiac arrest surveillance --- Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005--December 31, 2010.MMWR Surveill Summ. 2011 Jul 29;60(8):1-19. MMWR Surveill Summ. 2011. PMID: 21796098
-
Out-of-hospital airway management and cardiac arrest outcomes: a propensity score matched analysis.Resuscitation. 2012 Mar;83(3):313-9. doi: 10.1016/j.resuscitation.2011.10.028. Epub 2011 Nov 18. Resuscitation. 2012. PMID: 22101202
-
Association of the Emergency Medical Services-Related Time Interval with Survival Outcomes of Out-of-Hospital Cardiac Arrest Cases in Four Asian Metropolitan Cities Using the Scoop-and-Run Emergency Medical Services Model.J Emerg Med. 2017 Nov;53(5):688-696.e1. doi: 10.1016/j.jemermed.2017.08.076. J Emerg Med. 2017. PMID: 29128033
-
Community first responders for out-of-hospital cardiac arrest in adults and children.Cochrane Database Syst Rev. 2019 Jul 19;7(7):CD012764. doi: 10.1002/14651858.CD012764.pub2. Cochrane Database Syst Rev. 2019. PMID: 31323120 Free PMC article.
-
AI-Enabled Public Surveillance Cameras for Rapid Emergency Medical Service Activation in Out-of-Hospital Cardiac Arrests.Curr Probl Cardiol. 2023 Nov;48(11):101915. doi: 10.1016/j.cpcardiol.2023.101915. Epub 2023 Jun 30. Curr Probl Cardiol. 2023. PMID: 37392980 Review.
Cited by
-
Urban-Rural Differences in Cardiac Arrest Outcomes: A Retrospective Population-Based Cohort Study.CJC Open. 2021 Dec 30;4(4):383-389. doi: 10.1016/j.cjco.2021.12.010. eCollection 2022 Apr. CJC Open. 2021. PMID: 35495857 Free PMC article.
-
Demographic, social, economic and geographic factors associated with long-term outcomes in a cohort of cardiac arrest survivors.Resuscitation. 2018 Jul;128:31-36. doi: 10.1016/j.resuscitation.2018.04.032. Epub 2018 Apr 26. Resuscitation. 2018. PMID: 29705340 Free PMC article.
-
Spatio-temporal prediction model of out-of-hospital cardiac arrest: Designation of medical priorities and estimation of human resources requirement.PLoS One. 2020 Aug 31;15(8):e0238067. doi: 10.1371/journal.pone.0238067. eCollection 2020. PLoS One. 2020. PMID: 32866165 Free PMC article.
-
Spatiotemporal Analysis of Out-of-Hospital Cardiac Arrest Incidence and Survival Outcomes in Korea (2009-2021).J Korean Med Sci. 2024 Mar 11;39(9):e86. doi: 10.3346/jkms.2024.39.e86. J Korean Med Sci. 2024. PMID: 38469962 Free PMC article.
-
From Stadiums to Streets: Preventing Sudden Cardiac Death in Young Adults.J Am Heart Assoc. 2025 Jan 7;14(1):e038489. doi: 10.1161/JAHA.124.038489. Epub 2024 Dec 18. J Am Heart Assoc. 2025. PMID: 39692019 Free PMC article. No abstract available.
References
-
- McNally B, Robb R, Mehta M, Vellano K, Valderrama AL, Yoon P, et al. (2011) Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005—December 31, 2010. MMWR Surveill Summ 60: 1–19. - PubMed
-
- Atwood C, Eisenberg MS, Herlitz J, Rea TD (2005) Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 67: 75–80. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
