

A Multifaceted Strategy to Implement Brief Smoking Cessation Counseling During Antenatal Care in Argentina and Uruguay: A Cluster Randomized Trial
- PMID: 26660265
- PMCID: PMC4922364
- DOI: 10.1093/ntr/ntv276
A Multifaceted Strategy to Implement Brief Smoking Cessation Counseling During Antenatal Care in Argentina and Uruguay: A Cluster Randomized Trial
Abstract
Introduction: Argentina and Uruguay have a high prevalence of smoking during pregnancy. However, and despite national recommendations, pregnant women are not routinely receiving cessation counseling during antenatal care (ANC). We evaluated a multifaceted strategy designed to increase the frequency of pregnant women who received a brief smoking cessation counseling based on the 5As (Ask, Advise, Assess, Assist, and Arrange).
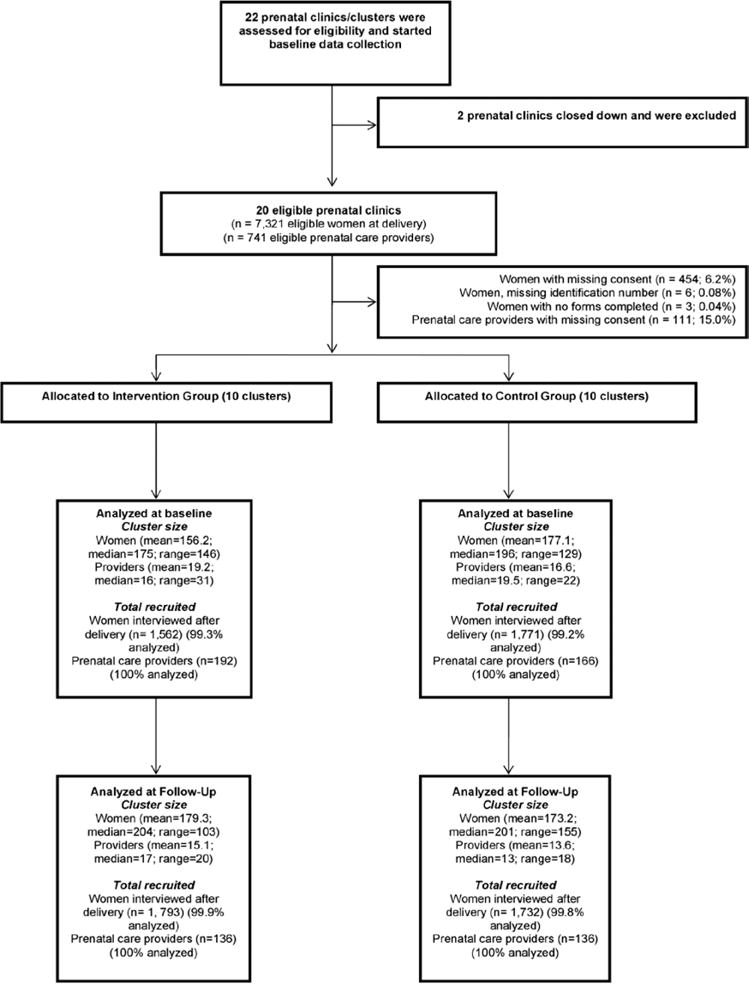
Methods: We randomly assigned (1:1) 20 ANC clusters in Buenos Aires, Argentina and Montevideo, Uruguay to receive a multifaceted intervention to implement brief smoking cessation counseling into routine ANC, or to receive no intervention. The primary outcome was the frequency of women who recalled receiving the 5As during ANC at more than one visit. Frequency of women who smoked until the end of pregnancy, and attitudes and readiness of ANC providers towards providing counseling were secondary outcomes. Women's outcomes were measured at baseline and at the end of the 14- to 18-month intervention, by administering questionnaires at the postpartum hospital stay. Self-reported cessation was verified with saliva cotinine. The trial took place between October 03, 2011 and November 29, 2013.
Results: The rate of women who recalled receiving the 5As increased from 14.0% to 33.6% in the intervention group (median rate change, 22.1%), and from 10.8% to 17.0% in the control group (median rate change, 4.6%; P = .001 for the difference in change between groups). The effect of the intervention was larger in Argentina than in Uruguay. The proportion of women who continued smoking during pregnancy was unchanged at follow-up in both groups and the relative difference between groups was not statistically significant (ratio of odds ratios 1.16, 95% CI: 0.98-1.37; P = .086). No significant changes were observed in knowledge, attitudes, and self-confidence of ANC providers.
Conclusions: The intervention showed a moderate effect in increasing the proportion of women who recalled receiving the 5As, with a third of women receiving counseling in more than one visit. However, the frequency of women who smoked until the end of the pregnancy was not significantly reduced by the intervention.
Implications: No implementation trials of smoking cessation interventions for pregnant women have been carried out in Latin American or in middle-income countries where health care systems or capacities may differ. We evaluated a multifaceted strategy designed to increase the frequency of pregnant women who receive brief smoking cessation counseling based on the 5As in Argentina and Uruguay. We found that the intervention showed a moderate effect in increasing the proportion of women receiving the 5As, with a third of women receiving counseling in more than one visit. However, the frequency of women who smoked until the end of the pregnancy was not significantly reduced by the intervention.
Published by Oxford University Press on behalf of the Society for Research on Nicotine and Tobacco 2015. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Conflict of interest statement
Declaration of Interests
Similar articles
-
Smoking Patterns and Receipt of Cessation Services Among Pregnant Women in Argentina and Uruguay.Nicotine Tob Res. 2016 May;18(5):1116-25. doi: 10.1093/ntr/ntv145. Epub 2015 Jun 27. Nicotine Tob Res. 2016. PMID: 26117836 Free PMC article.
-
Tobacco cessation intervention for pregnant women in Argentina and Uruguay: study protocol.Reprod Health. 2013 Aug 26;10(1):44. doi: 10.1186/1742-4755-10-44. Reprod Health. 2013. PMID: 23971512 Free PMC article. Clinical Trial.
-
Barriers and promoters of an evidenced-based smoking cessation counseling during prenatal care in Argentina and Uruguay.Matern Child Health J. 2015 Jul;19(7):1481-9. doi: 10.1007/s10995-014-1652-3. Matern Child Health J. 2015. PMID: 25500989 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Provision and uptake of routine antenatal services: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2019 Jun 12;6(6):CD012392. doi: 10.1002/14651858.CD012392.pub2. Cochrane Database Syst Rev. 2019. PMID: 31194903 Free PMC article.
Cited by
-
Improving smoking cessation care in pregnancy at Aboriginal Medical Services: 'ICAN QUIT in Pregnancy' step-wedge cluster randomised study.BMJ Open. 2019 Jun 4;9(6):e025293. doi: 10.1136/bmjopen-2018-025293. BMJ Open. 2019. PMID: 31167863 Free PMC article. Clinical Trial.
-
Syphilis screening and treatment in pregnant women in Kinshasa, Democratic Republic of the Congo and in Lusaka, Zambia: a cross-sectional study.Gates Open Res. 2017 Dec 8;1:13. doi: 10.12688/gatesopenres.12768.1. Gates Open Res. 2017. PMID: 29355227 Free PMC article.
-
Behavioral Interventions for Tobacco Cessation in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis.Nicotine Tob Res. 2025 Mar 24;27(4):575-585. doi: 10.1093/ntr/ntae259. Nicotine Tob Res. 2025. PMID: 39485008 Free PMC article.
-
Prevalence and patterns of cigarette smoking before and during early and late pregnancy according to maternal characteristics: the first national data based on the 2003 birth certificate revision, United States, 2016.Reprod Health. 2019 Sep 13;16(1):142. doi: 10.1186/s12978-019-0807-5. Reprod Health. 2019. PMID: 31519184 Free PMC article.
-
Barriers and facilitators to smoking cessation in pregnancy and in the post-partum period: The health care professionals' perspective.Br J Health Psychol. 2018 Sep;23(3):741-757. doi: 10.1111/bjhp.12314. Epub 2018 May 15. Br J Health Psychol. 2018. PMID: 29766615 Free PMC article.
References
-
- World Health Organization. WHO Recommendations for the Prevention and Management of Tobacco Use and Second-hand Smoke Exposure in Pregnancy. Geneva, Switzerland: World Health Organization; 2013. www.who.int/tobacco/publications/pregnancy/guidelinestobaccosmokeexposur.... Accessed January 26, 2015. - PubMed
-
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
-
- World Health Organization. International Consultation on Environmental Tobacco Smoke (ETS) and Child Health. Geneva, Switzerland: World Health Organization; 1999.
-
- Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
