

Stroke neuroprotection revisited: Intra-arterial verapamil is profoundly neuroprotective in experimental acute ischemic stroke
- PMID: 26661189
- PMCID: PMC4821022
- DOI: 10.1177/0271678X15608395
Stroke neuroprotection revisited: Intra-arterial verapamil is profoundly neuroprotective in experimental acute ischemic stroke
Abstract
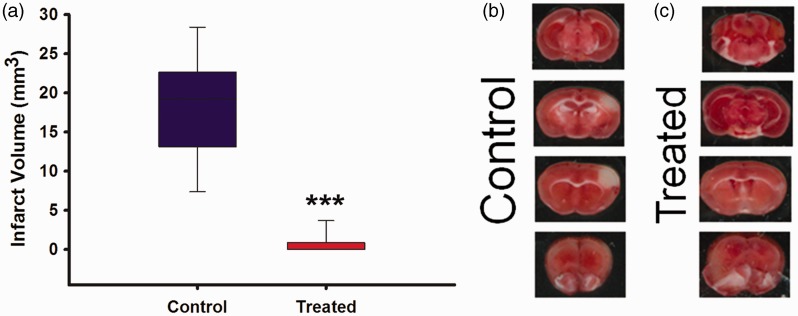
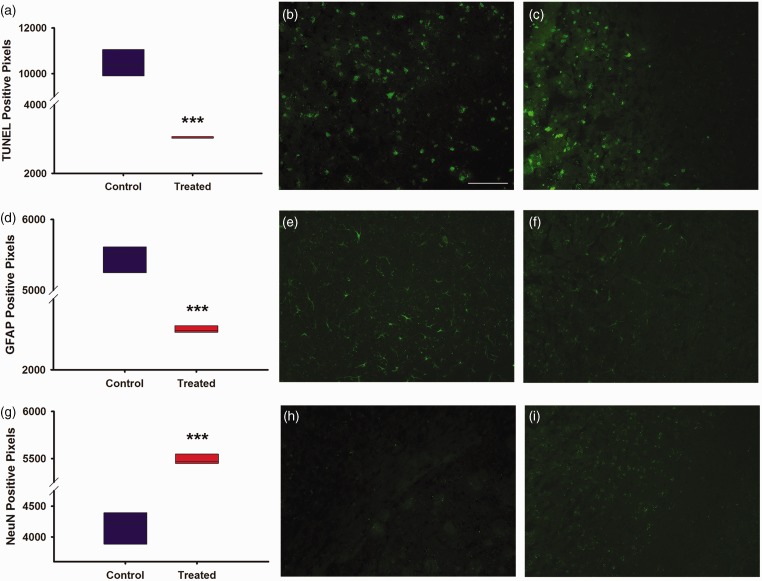
While clinical trials have now solidified the role of thrombectomy in emergent large vessel occlusive stroke, additional therapies are needed to optimize patient outcome. Using our previously described experimental ischemic stroke model for evaluating adjunctive intra-arterial drug therapy after vessel recanalization, we studied the potential neuroprotective effects of verapamil. A calcium channel blocker, verapamil is often infused intra-arterially by neurointerventionalists to treat cerebral vasospasm. Such a direct route of administration allows for both focused targeting of stroke-impacted brain tissue and minimizes potential systemic side effects. Intra-arterial administration of verapamil at a flow rate of 2.5 µl/min and injection volume of 10 µl immediately after middle cerebral artery recanalization in C57/Bl6 mice was shown to be profoundly neuroprotective as compared to intra-arterial vehicle-treated stroke controls. Specifically, we noted a significant (P ≤ 0.05) decrease in infarct volume, astrogliosis, and cellular apoptosis as well as a significant increase in neuronal survival and functional outcome over seven days. Furthermore, intra-arterial administration of verapamil was well tolerated with no hemorrhage, systemic side effects, or increased mortality. Thus, verapamil administered intra-arterially immediately following recanalization in experimental ischemic stroke is both safe and neuroprotective and merits further study as a potential therapeutic adjunct to thrombectomy.
Keywords: Ischemic stroke; cerebral ischemia; intra-arterial; neuroprotection; recanalization; verapamil.
© The Author(s) 2015.
Figures
References
-
- Saver JL, Jahan R, Levy EI, et al. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet 2012; 380: 1241–1249. - PubMed
-
- Bretz MN, Graves A, West A, et al. Steps against recurrent stroke plus: patient transition program. J Neurosci Nurs 2014; 46: E3–13. quiz E1-2. - PubMed
-
- Thacker C. Stroke falls to No. 5 cause of death in U.S. American Heart Association Media Alert. 12/30/2014 ed2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
