

The impact of the introduction of fidaxomicin on the management of Clostridium difficile infection in seven NHS secondary care hospitals in England: a series of local service evaluations
- PMID: 26661400
- PMCID: PMC4724367
- DOI: 10.1007/s10096-015-2538-z
The impact of the introduction of fidaxomicin on the management of Clostridium difficile infection in seven NHS secondary care hospitals in England: a series of local service evaluations
Abstract
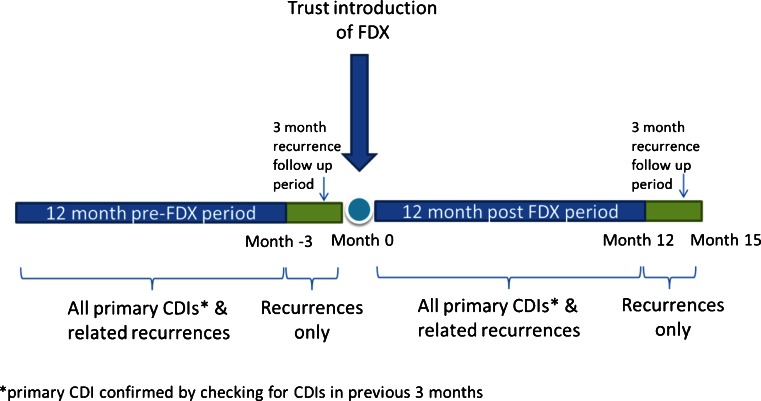
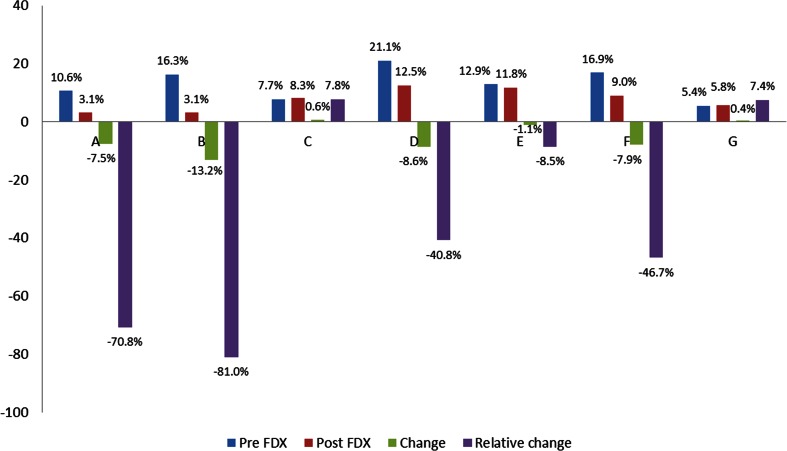
Clostridium difficile infection (CDI) is associated with high mortality. Reducing incidence is a priority for patients, clinicians, the National Health Service (NHS) and Public Health England alike. In June 2012, fidaxomicin (FDX) was launched for the treatment of adults with CDI. The objective of this evaluation was to collect robust real-world data to understand the effectiveness of FDX in routine practice. In seven hospitals introducing FDX between July 2012 and July 2013, data were collected retrospectively from medical records on CDI episodes occurring 12 months before/after the introduction of FDX. All hospitalised patients aged ≥18 years with primary CDI (diarrhoea with presence of toxin A/B without a previous CDI in the previous 3 months) were included. Recurrence was defined as in-patient diarrhoea re-emergence requiring treatment any time within 3 months after the first episode. Each hospital had a different protocol for the use of FDX. In hospitals A and B, where FDX was used first line for all primary and recurrent episodes, the recurrence rate reduced from 10.6 % to 3.1 % and from 16.3 % to 3.1 %, with a significant difference in 28-day mortality from 18.2 % to 3.1 % (p < 0.05) and 17.3 % to 6.3 % (p < 0.05) for hospitals A and B, respectively. In hospitals using FDX in selected patients only, the changes in recurrence rates and mortality were less marked. The pattern of adoption of FDX appears to affect its impact on CDI outcome, with maximum reduction in recurrence and all-cause mortality where it is used as first-line treatment.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
