

Assessing race and ethnicity data quality across cancer registries and EMRs in two hospitals
- PMID: 26661718
- PMCID: PMC6095103
- DOI: 10.1093/jamia/ocv156
Assessing race and ethnicity data quality across cancer registries and EMRs in two hospitals
Abstract
Background: Measurement of patient race/ethnicity in electronic health records is mandated and important for tracking health disparities.
Objective: Characterize the quality of race/ethnicity data collection efforts.
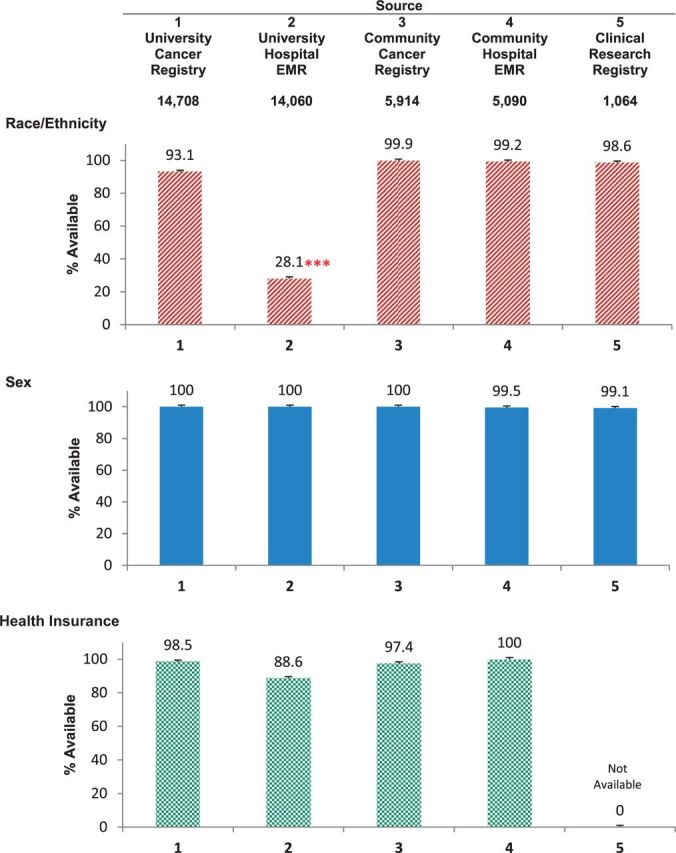
Methods: For all cancer patients diagnosed (2007-2010) at two hospitals, we extracted demographic data from five sources: 1) a university hospital cancer registry, 2) a university electronic medical record (EMR), 3) a community hospital cancer registry, 4) a community EMR, and 5) a joint clinical research registry. The patients whose data we examined (N = 17 834) contributed 41 025 entries (range: 2-5 per patient across sources), and the source comparisons generated 1-10 unique pairs per patient. We used generalized estimating equations, chi-squares tests, and kappas estimates to assess data availability and agreement.
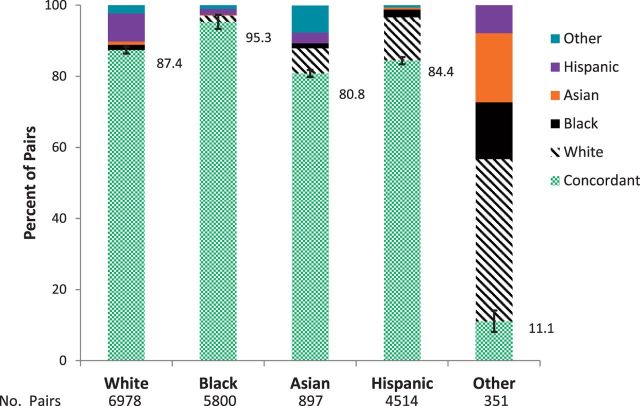
Results: Compared to sex and insurance status, race/ethnicity information was significantly less likely to be available (χ(2 )> 8043, P < .001), with variation across sources (χ(2 )> 10 589, P < .001). The university EMR had a high prevalence of "Unknown" values. Aggregate kappa estimates across the sources was 0.45 (95% confidence interval, 0.45-0.45; N = 31 276 unique pairs), but improved in sensitivity analyses that excluded the university EMR source (κ = 0.89). Race/ethnicity data were in complete agreement for only 6988 patients (39.2%). Pairs with a "Black" data value in one of the sources had the highest agreement (95.3%), whereas pairs with an "Other" value exhibited the lowest agreement across sources (11.1%).
Discussion: Our findings suggest that high-quality race/ethnicity data are attainable. Many of the "errors" in race/ethnicity data are caused by missing or "Unknown" data values.
Conclusions: To facilitate transparent reporting of healthcare delivery outcomes by race/ethnicity, healthcare systems need to monitor and enforce race/ethnicity data collection standards.
Keywords: cancer registry; data quality; electronic medical record; race and ethnicity.
© The Author 2015. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
