

Postoperative Complications, In-Hospital Mortality and 5-Year Survival After Surgical Resection for Patients with a Pancreatic Neuroendocrine Tumor: A Systematic Review
- PMID: 26661846
- PMCID: PMC4746219
- DOI: 10.1007/s00268-015-3328-6
Postoperative Complications, In-Hospital Mortality and 5-Year Survival After Surgical Resection for Patients with a Pancreatic Neuroendocrine Tumor: A Systematic Review
Abstract
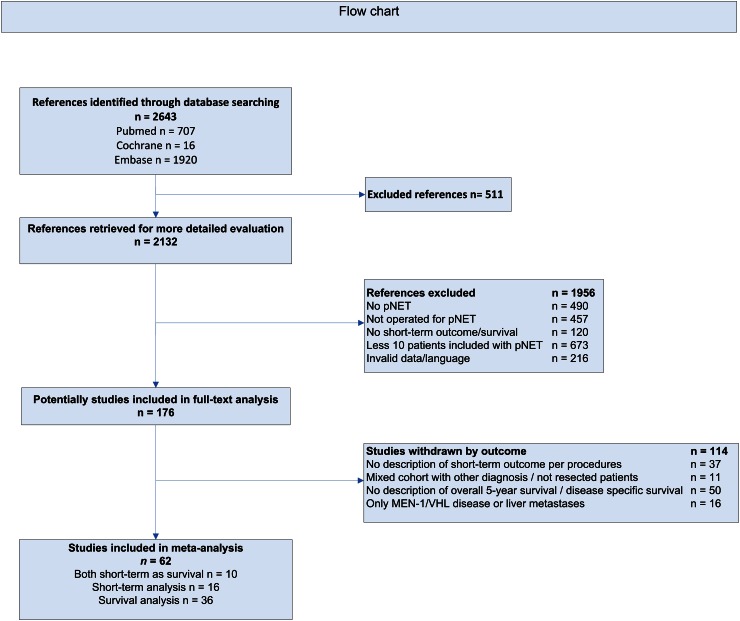
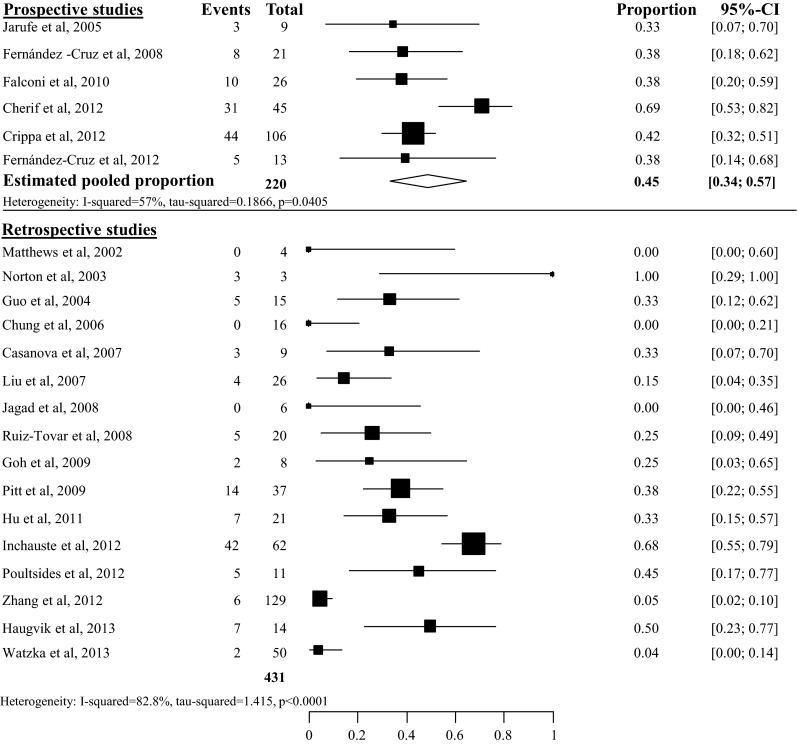
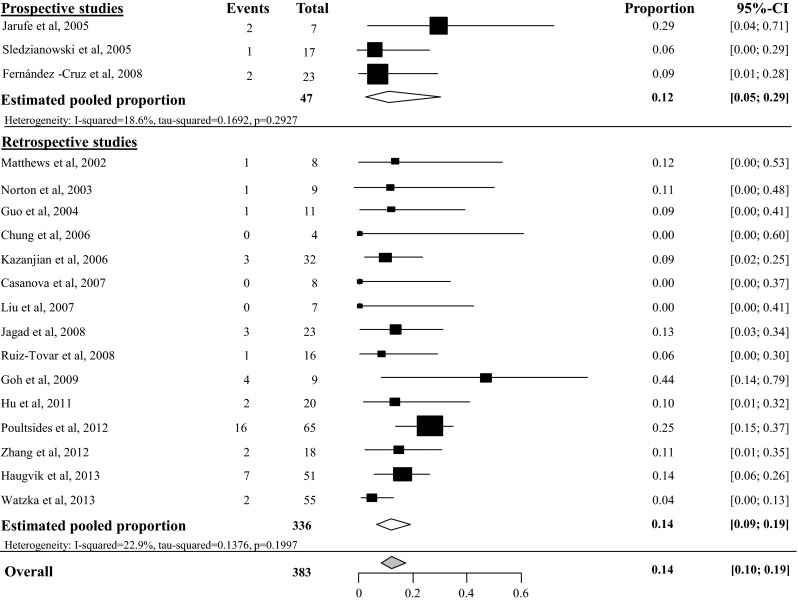
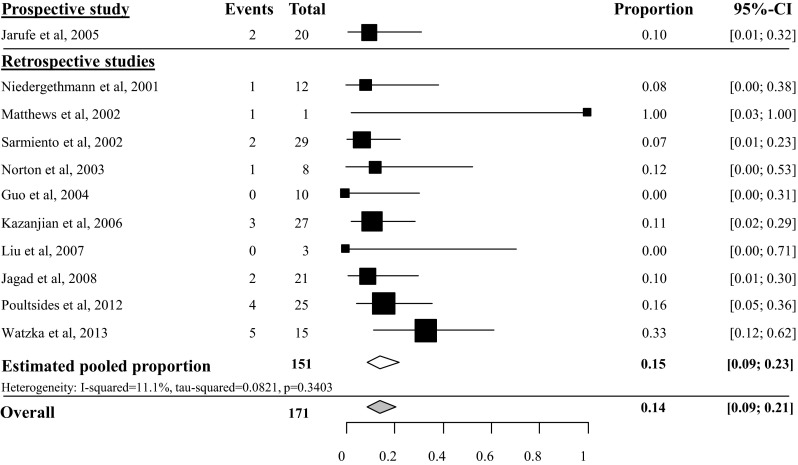
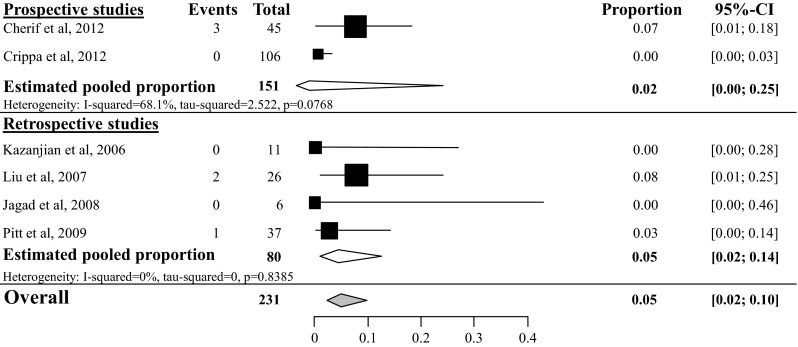
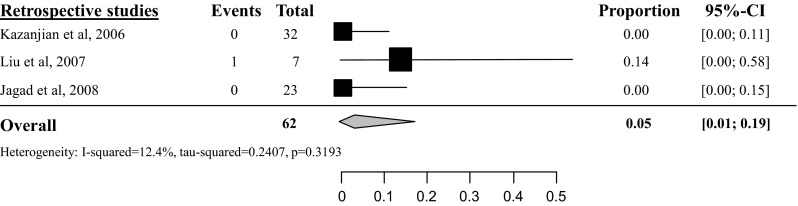
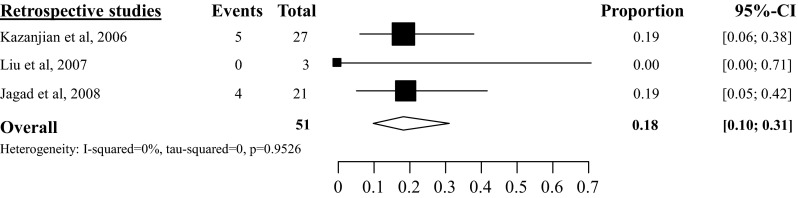
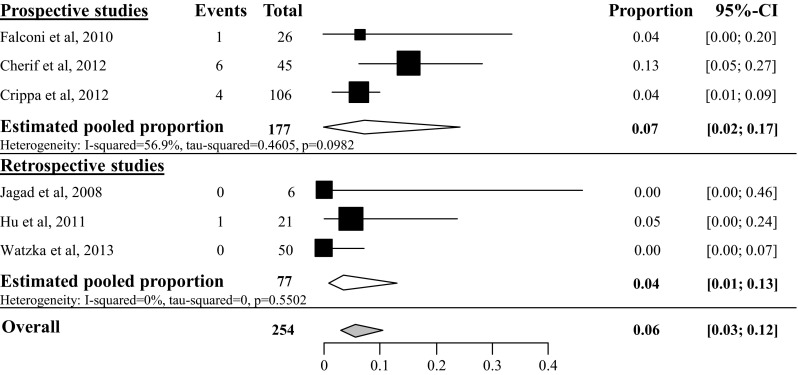
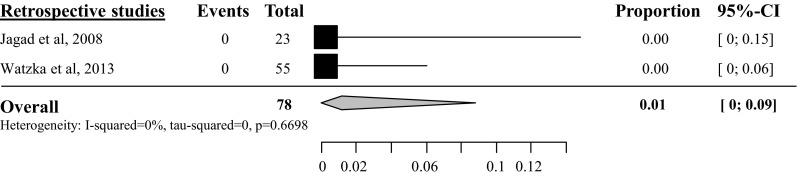
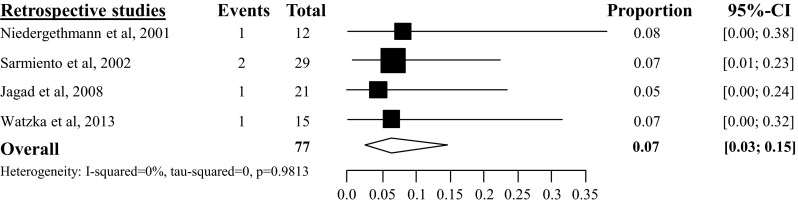
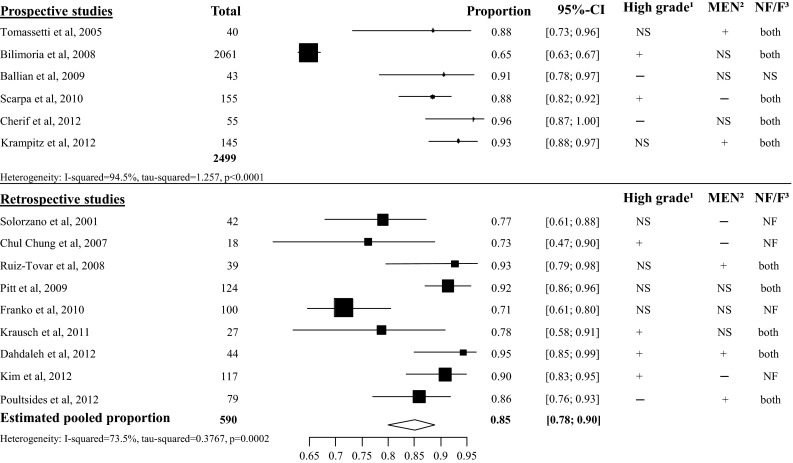
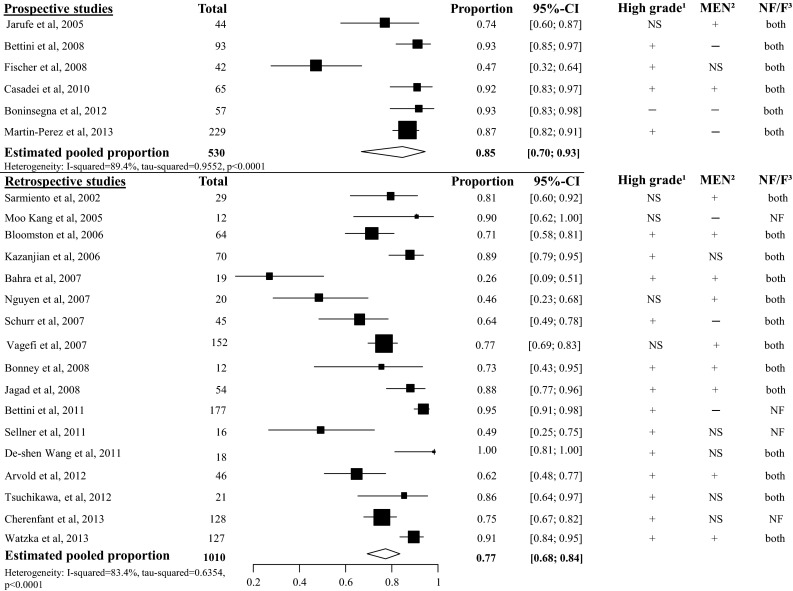
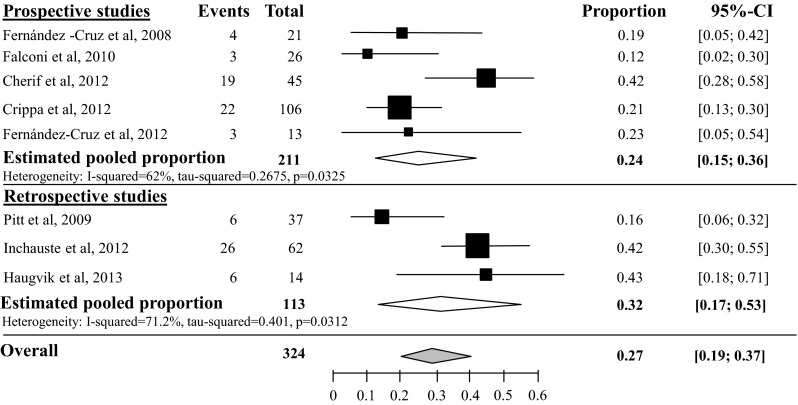
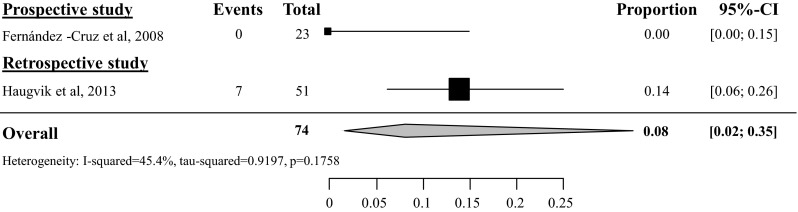
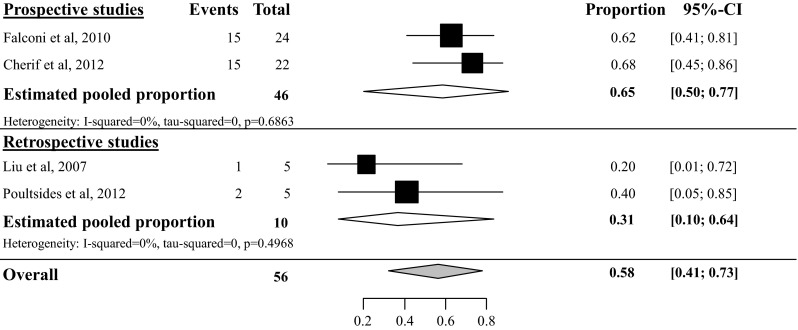
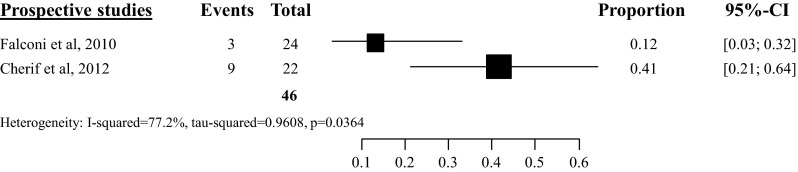
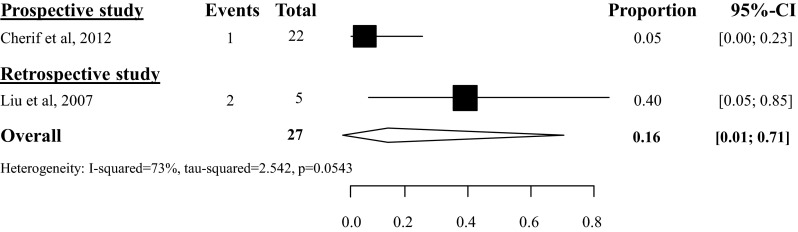
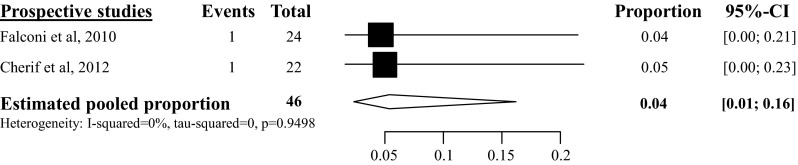
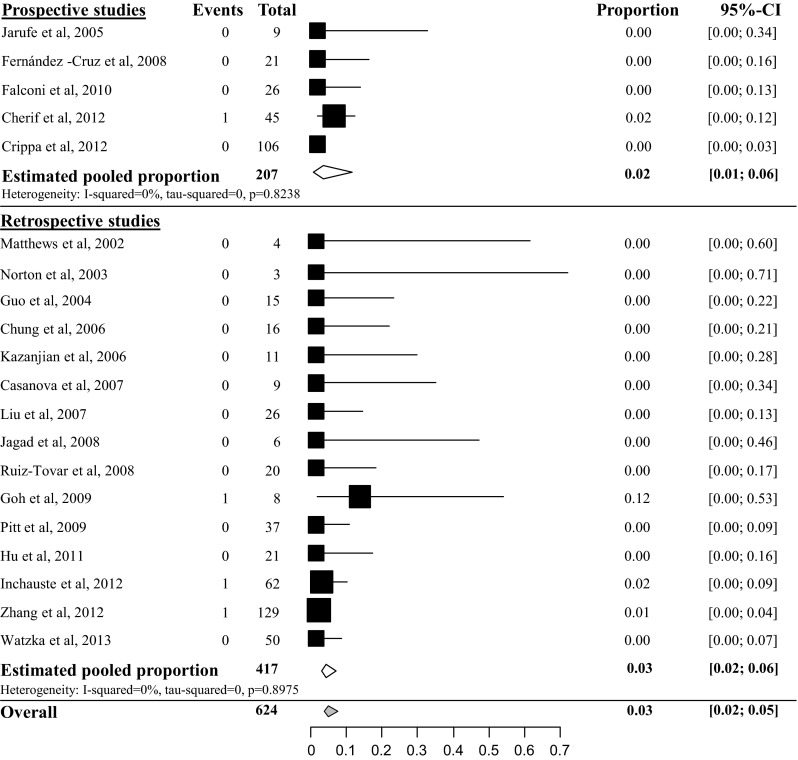
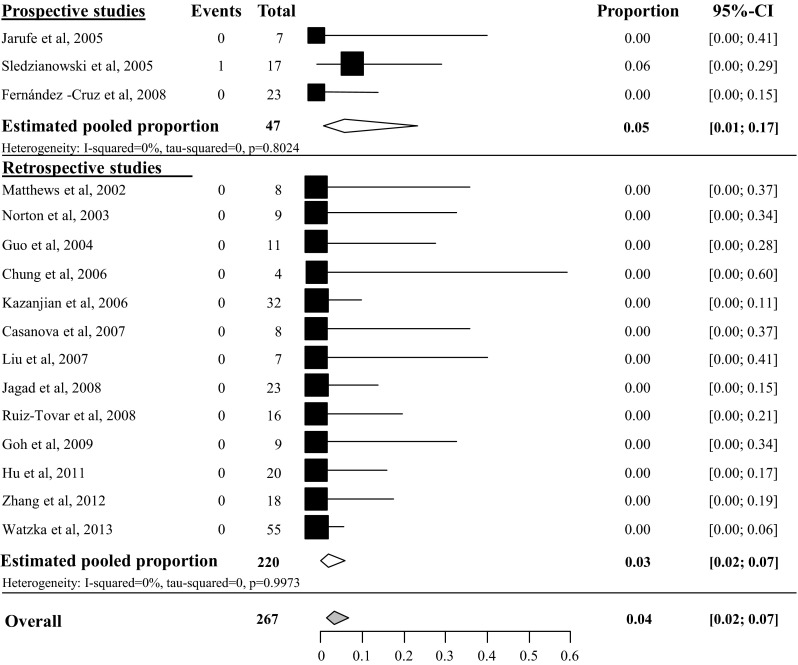
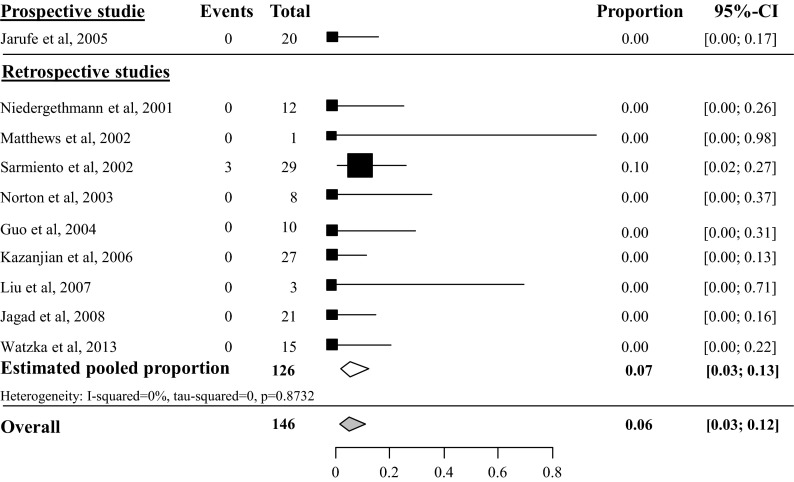
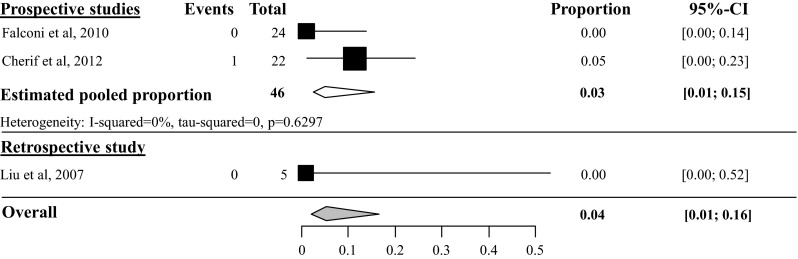
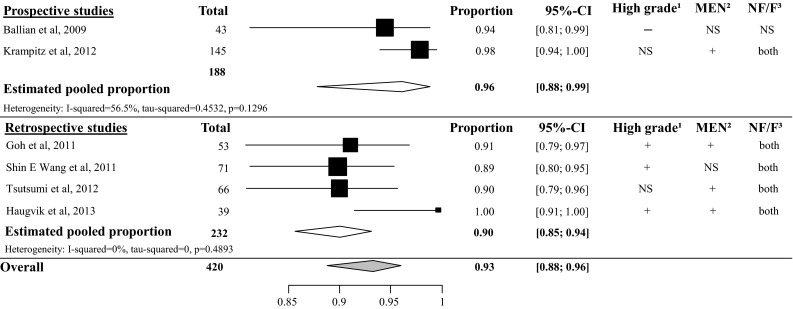
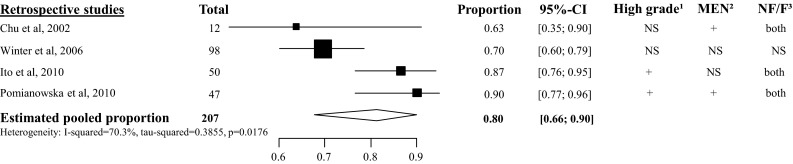
Studies on postoperative complications and survival in patients with pancreatic neuroendocrine tumors (pNET) are sparse and randomized controlled trials are not available. We reviewed all studies on postoperative complications and survival after resection of pNET. A systematic search was performed in the Cochrane Central Register of Controlled Trials, MEDLINE and EMBASE from 2000-2013. Inclusion criteria were studies of resected pNET, which described postoperative complications separately for each surgical procedure and/or 5-year survival after resection. Prospective and retrospective studies were pooled separately and overall pooled if heterogeneity was below 75%. The random-effect model was used. Overall, 2643 studies were identified and after full-text analysis 62 studies were included. Pancreatic fistula (PF) rate of the prospective studies after tumor enucleation was 45%; PF-rates after distal pancreatectomy, pancreatoduodenectomy, or central pancreatectomy were, respectively, 14-14-58%. Delayed gastric emptying rates were, respectively, 5-5-18-16%. Postoperative hemorrhage rates were, respectively, 6-1-7-4%. In-hospital mortality rates were, respectively, 3-4-6-4%. The 5-year overall survival (OS) and disease-specific survival (DSS) of resected pNET without synchronous resected liver metastases were, respectively, 85-93%. Heterogeneity between included studies on 5-year OS in patients with synchronous resected liver metastases was too high to pool all studies. The 5-year DSS in patients with liver metastases was 80%. Morbidity after pancreatic resection for pNET was mainly caused by PF. Liver resection in patients with liver metastases seems to have a positive effect on DSS. To reduce heterogeneity, ISGPS criteria and uniform patient groups should be used in the analysis of postoperative outcome and survival.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
