

Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour
- PMID: 26662716
- PMCID: PMC8697562
- DOI: 10.1002/14651858.CD011200.pub2
Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour
Abstract
Background: Magnesium sulphate has been used to inhibit preterm labour to prevent preterm birth. There is no consensus as to the safety profile of different treatment regimens with respect to dose, duration, route and timing of administration.
Objectives: To assess the efficacy and safety of alternative magnesium sulphate regimens when used as single agent tocolytic therapy during pregnancy.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (30 September 2015) and reference lists of retrieved studies.
Selection criteria: Randomised trials comparing different magnesium sulphate treatment regimens when used as single agent tocolytic therapy during pregnancy in women in preterm labour. Quasi-randomised trials were eligible for inclusion but none were identified. Cross-over and cluster trials were not eligible for inclusion. Health outcomes were considered at the level of the mother, the infant/child and the health service.
Intervention: intravenous or oral magnesium sulphate given alone for tocolysis.Comparison: alternative dosing regimens of magnesium sulphate given alone for tocolysis.
Data collection and analysis: Two review authors independently assessed trial eligibility and quality and extracted data.
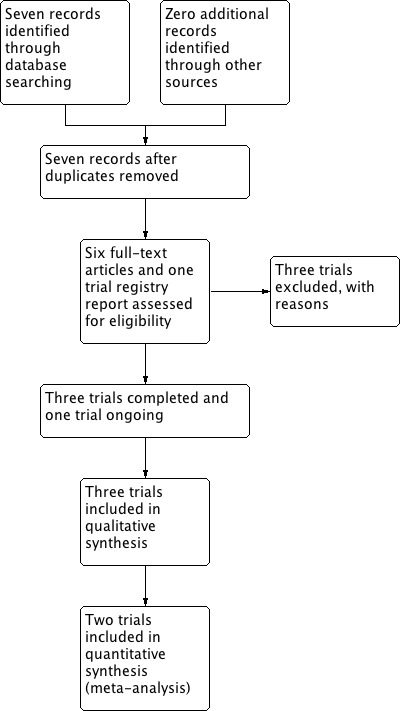
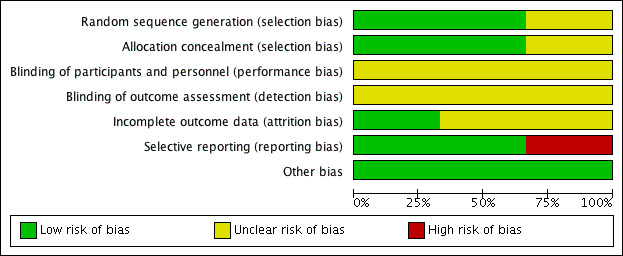
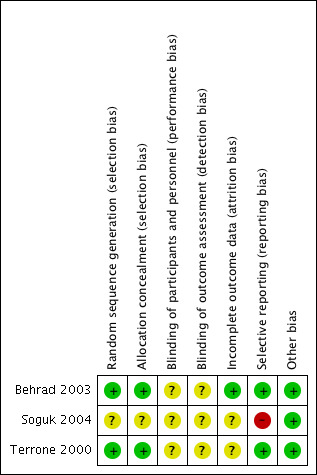
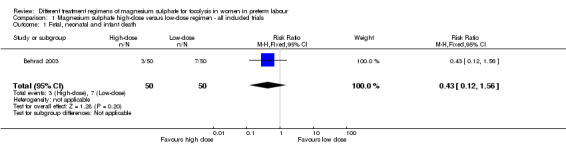
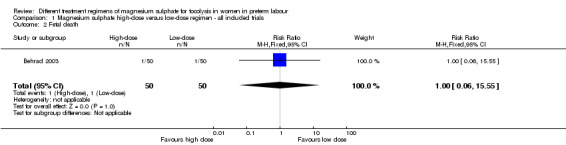
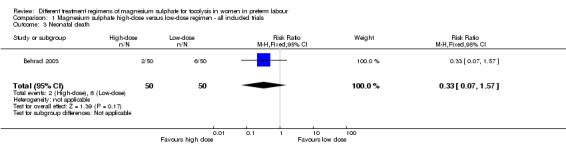
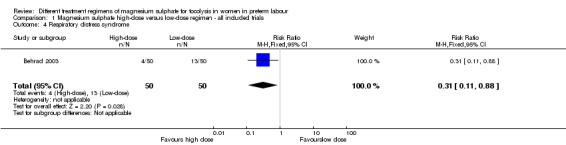
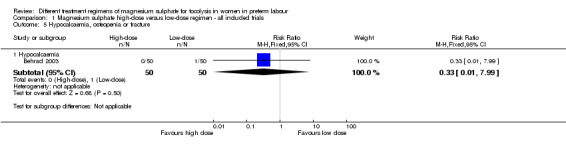
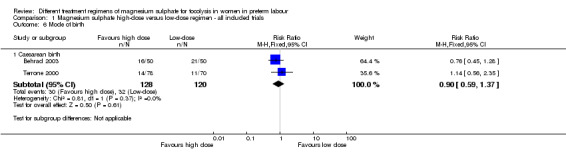
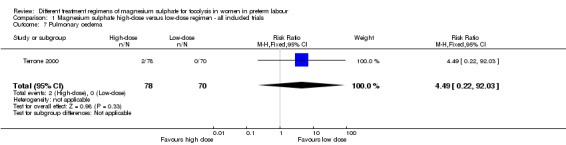
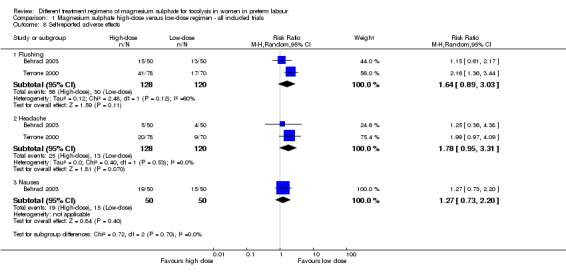
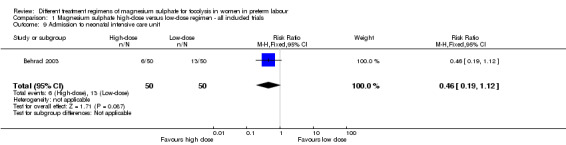
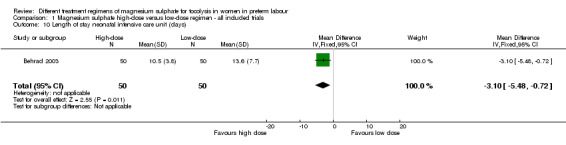
Main results: Three trials including 360 women and their infants were identified as eligible for inclusion in this review. Two trials were rated as low risk of bias for random sequence generation and concealment of allocation. A third trial was assessed as unclear risk of bias for these domains but did not report data for any of the outcomes examined in this review. No trials were rated to be of high quality overall.Intravenous magnesium sulphate was administered according to low-dose regimens (4 g loading dose followed by 2 g/hour continuous infusion and/or increased by 1 g/hour hourly until successful tocolysis or failure of treatment), or high-dose regimens (4 g loading dose followed by 5 g/hour continuous infusion and increased by 1 g/hour hourly until successful tocolysis or failure of treatment, or 6 g loading dose followed by 2 g/hour continuous infusion and increased by 1 g/hour hourly until successful tocolysis or failure of treatment).There were no differences seen between high-dose magnesium sulphate regimens compared with low-dose magnesium sulphate regimens for the primary outcome of fetal, neonatal and infant death (risk ratio (RR) 0.43, 95% confidence interval (CI) 0.12 to 1.56; one trial, 100 infants). Using the GRADE approach, the evidence for fetal, neonatal and infant death was considered to be VERY LOW quality. No data were reported for any of the other primary maternal and infant health outcomes (birth less than 48 hours after trial entry; composite serious infant outcome; composite serious maternal outcome).There were no clear differences seen between high-dose magnesium sulphate regimens compared with low-dose magnesium sulphate regimens for the secondary infant health outcomes of fetal death; neonatal death; and rate of hypocalcaemia, osteopenia or fracture; and secondary maternal health outcomes of rate of caesarean birth; pulmonary oedema; and maternal self-reported adverse effects. Pulmonary oedema was reported in two women given high-dose magnesium sulphate, but not in any of the women given low-dose magnesium sulphate.In a single trial of high and low doses of magnesium sulphate for tocolysis including 100 infants, the risk of respiratory distress syndrome was lower with use of a high-dose regimen compared with a low-dose regimen (RR 0.31, 95% CI 0.11 to 0.88; one trial, 100 infants). Using the GRADE approach, the evidence for respiratory distress syndrome was judged to be LOW quality. No difference was seen in the rate of admission to the neonatal intensive care unit. However, for those babies admitted, a high-dose regimen was associated with a reduction in the length of stay in the neonatal intensive care unit compared with a low-dose regimen (mean difference -3.10 days, 95% confidence interval -5.48 to -0.72).We found no data for the majority of our secondary outcomes.
Authors' conclusions: There are limited data available (three studies, with data from only two studies) comparing different dosing regimens of magnesium sulphate given as single agent tocolytic therapy for the prevention of preterm birth. There is no evidence examining duration of therapy, timing of therapy and the role for repeat dosing.Downgrading decisions for our primary outcome of fetal, neonatal and infant death were based on wide confidence intervals (crossing the line of no effect), lack of blinding and a limited number of studies. No data were available for any of our other important outcomes: birth less than 48 hours after trial entry; composite serious infant outcome; composite serious maternal outcome. The data are limited by volume and the outcomes reported. Only eight of our 45 pre-specified primary and secondary maternal and infant health outcomes were reported on in the included studies. No long-term outcomes were reported. Downgrading decisions for the evidence on the risk of respiratory distress were based on wide confidence intervals (crossing the line of no effect) and lack of blinding.There is some evidence from a single study suggesting a reduction in the length of stay in the neonatal intensive care unit and a reduced risk of respiratory distress syndrome where a high-dose regimen of magnesium sulphate has been used compared with a low-dose regimen. However, given that evidence has been drawn from a single study (with a small sample size), these data should be interpreted with caution.Magnesium sulphate has been shown to be of benefit in a wide range of obstetric settings, although it has not been recommended for tocolysis. In clinical settings where health benefits are established, further trials are needed to address the lack of evidence regarding the optimal dose (loading dose and maintenance dose), duration of therapy, timing of therapy and role for repeat dosing in terms of efficacy and safety for mothers and their children. Ongoing examination of different regimens with respect to important health outcomes is required.
Conflict of interest statement
Helen C McNamara: none known
Caroline A Crowther: none known
Julie Brown: none known
Figures
Update of
References
References to studies included in this review
Behrad 2003 {published data only}
-
- Behrad V, Moossavifar N, Mojtahedzadeh M, Esmalli H, Moghtadeli P. A prospective, randomized, controlled trial of high and low doses of magnesium sulfate for acute tocolysis. Acta Medica Iranica 2003;41(2):126‐31.
Soguk 2004 {published data only}
-
- Soguk C, Tapisiz OL, Mungan T. Low dose treatment protocol in magnesium sulfate tocolysis. International Journal of Gynecology & Obstetrics 2004;86:37‐8. - PubMed
Terrone 2000 {published data only}
-
- Terrone DA, Rinehart BK, Kimmel ES, May WL, Larmon JE, Morrison JC. A prospective, randomized, controlled trial of high and low maintenance doses of magnesium sulfate for acute tocolysis. American Journal of Obstetrics and Gynecology 2000;182(6):1477‐82. - PubMed
References to studies excluded from this review
Martin 1990 {published data only}
-
- Martin RW, Perry KG, Martin JN, Hess LW, Morrison JC. Oral magnesium for tocolysis: a comparison of magnesium gluconate and enteric‐coated magnesium chloride. Proceedings of 37th Annual Meeting of the Society for Gynecologic Investigation; 1990 March 21‐24; St Louis, USA. 1990:167.
Martin 1998 {published data only}
-
- Martin RW, Perry KGJ, Martin JN, Seago DP, Roberts WE, Morrison JC. Oral magnesium for tocolysis: a comparison of magnesium gluconate and enteric‐coated magnesium chloride. Journal of the Mississippi State Medical Association 1998;39(5):180‐2. - PubMed
Zygmunt 2003 {published data only}
-
- Zygmunt M, Heilmann L, Berg C, Wallwiener D, Grischke E, Munstedt K, et al. Local and systemic tolerability of magnesium sulphate for tocolysis. European Journal of Obstetrics & Gynecology and Reproductive Biology 2003;107(2):168‐75. - PubMed
References to ongoing studies
Namazi 2013 {published data only}
-
- Namazi SS. Comparison of maintenance therapy and continuous intravenous therapy with magnesium sulfate in preterm labor pain management at 24‐36 weeks gestation: a randomized controlled trial. IRCT Iranian Registry of Clinical Trials (www.irct.ir) [accessed 10 January 2015].
Additional references
Abarbanel 1945
-
- Abarbanel, AR. The spasmolysant action of magnesium ions on the tetanically contracting human gravid uterus. American Journal of Obstetrics and Gynecology 1945;49(4):473‐83.
ACOG 2012
-
- ACOG. ACOG Practice Bulletin. Clinical management guidelines for obstetrician‐gynecologists. Number 127, June 2012. Management of preterm labor. Obstetrics & Gynecology 2012; Vol. 119:1308‐17.
Bain 2012
Bain 2013
Beck 2010
Borna 2007
-
- Borna S, Saeidi FM. Celecoxib versus magnesium sulfate to arrest preterm labor: randomized trial. Journal of Obstetrics and Gynaecology Research 2007;33(5):631‐4. - PubMed
Borna 2008
-
- Borna S, Sahabi N. Progesterone for maintenance tocolytic therapy after threatened preterm labour: a randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2008;48(1):58‐63. - PubMed
Crowther 2014
Dowling 2012
-
- Dowling O, Chatterjee PK, Gupta M, Tam Tam HB, Xue X, Lewis D, et al. Magnesium sulfate reduces bacterial LPS‐induced inflammation at the maternal‐fetal interface. Placenta 2012;33(5):392‐8. - PubMed
Doyle 2009
Duley 2010a
Duley 2010b
Duley 2010c
Duley 2010d
FDA 2013
-
- FDA, U.S. Food, Drug Administration. FDA Recommends against prolonged use of magnesium sulfate to stop pre‐term labour due to bone changes in exposed babies. Drug Safety Communications, U.S. Food and Drug Administration 2013.
Flenady 2014a
Flenady 2014b
Glock 1993
-
- Glock JL, Morales WJ. Efficacy and safety of nifedipine versus magnesium sulfate in the management of preterm labor: a randomized study. American Journal of Obstetrics and Gynecology 1993;169(4):960‐4. - PubMed
Goldenberg 2008
Grimes 2006
-
- Grimes DA, Nanda K. Magnesium sulfate tocolysis: time to quit. Obstetrics & Gynecology 2006;108(4):986‐9. - PubMed
Haas 2012
Haghighi 1999
-
- Haghighi L. Prevention of preterm delivery: nifedipine or magnesium sulfate. International Journal of Gynaecology and Obstetrics 1999;66(3):297‐8. - PubMed
Hall 1957
-
- Hall DG. Serum magnesium in pregnancy. Obstetrics & Gynecology 1957;9(2):158‐62. - PubMed
Han 2013
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
How 2006
-
- How HY, Zafaranchi L, Stella CL, Recht K, Maxwell RA, Sibai B, et al. Tocolysis in women with preterm labor between 32 0/7 and 34 6/7 weeks of gestation: a randomized controlled pilot study. American Journal of Obstetrics and Gynecology 2006;194(4):976‐81. - PubMed
James 2010
-
- James MF. Magnesium in obstetrics. Best Practice and Research Clinical Obstetrics and Gynaecology 2010;24(3):327‐37. - PubMed
Klauser 2012
-
- Klauser CK, Briery CM, Keiser SD, Martin RW, Kosek MA, Morrison JC. Effect of antenatal tocolysis on neonatal outcomes. Journal of Maternal Fetal & Neonatal Medicine 2012;25(12):2778‐81. - PubMed
Larmon 1999
-
- Larmon JE, Ross BS, May WL, Dickerson GA, Fischer RG, Morrison JC. Oral nicardipine versus intravenous magnesium sulfate for the treatment of preterm labor. American Journal of Obstetrics and Gynecology 1999;181(6):1432‐7. - PubMed
Lewis 2005
-
- Lewis DF. Magnesium sulfate: the first‐line tocolytic. Obstetrics and Gynecology Clinics of North America 2005;32(3):485‐500. - PubMed
Lurie 2004
-
- Lurie S, Gur D, Sadan O, Glezerman M. Relationship between uterine contractions and serum magnesium levels in patients treated for threatened preterm labour with intravenous magnesium sulphate. Journal of Obstetrics and Gynaecology 2004;24(3):247‐8. - PubMed
Lyell 2007
-
- Lyell DJ, Pullen K, Campbell L, Ching S, Druzin ML, Chitkara U, et al. Magnesium sulfate compared with nifedipine for acute tocolysis of preterm labor: a randomized controlled trial. Obstetrics & Gynecology 2007;110(1):61‐7. - PubMed
McWhorter 2004
-
- McWhorter J, Carlan SJ, O'Leary TD, Richichi K, O'Brien WF. Rofecoxib versus magnesium sulfate to arrest preterm labor: a randomized trial. Obstetrics & Gynecology 2004;103(5 Pt 1):923‐30. - PubMed
Mittendorf 1997
-
- Mittendorf R, Covert R, Boman J, Khoshnood B, Lee K, Siegler M. Is tocolytic magnesium sulphate associated with increased total paediatric mortality?. Lancet 1997;350(9090):1517‐8. - PubMed
Morales 1993
-
- Morales WJ, Madhav H. Efficacy and safety of indomethacin compared with magnesium sulfate in the management of preterm labor: a randomized study. American Journal of Obstetrics and Gynecology 1993;169(1):97‐102. - PubMed
Nassar 2006
-
- Nassar AH, Sakhel K, Maarouf H, Naassan GR, Usta IM. Adverse maternal and neonatal outcome of prolonged magnesium sulfate tocolysis. Acta Obstetricia et Gynecologica Scandinavica 2006;85(9):1099‐103. - PubMed
Neilson 2014
Pryde 2009
-
- Pryde PG, Mittendorf R. Contemporary usage of obstetric magnesium sulfate: indication, contraindication, and relevance of dose. Obstetrics & Gynecology 2009;114(3):669‐73. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schorr 1997
-
- Schorr SJ. Ketorolac is a safe and effective drug for acute tocolysis. Acta Diabetologica Latina 1997;176:S7.
Steer 1977
-
- Steer CM, Petrie RH. A comparison of magnesium sulfate and alcohol for the prevention of premature labor. American Journal of Obstetrics and Gynecology 1977;129(1):1‐4. - PubMed
Tam Tam 2011
-
- Tam Tam HB, Dowling O, Xue X, Lewis D, Rochelson B, Metz CN. Magnesium sulfate ameliorates maternal and fetal inflammation in a rat model of maternal infection. American Journal of Obstetrics and Gynecology 2011;204(4):364.e1‐364.e8. - PubMed
Tsatsaris 2004
-
- Tsatsaris V, Cabrol D, Carbonne B. Pharmacokinetics of tocolytic agents. Clinical Pharmacokinetics 2004;43(13):833‐44. - PubMed
WHO 1992
-
- World Health Organization. Pregnancy, childbirth and the puerperium. http://www.who.int/classifications/icd/en/ [accessed 24 May 2011] 1992.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical