

Hemophagocytic lymphohistiocytosis: An unusual complication in disseminated Mycobacterium tuberculosis
- PMID: 26664166
- PMCID: PMC4663863
- DOI: 10.4103/0970-2113.168100
Hemophagocytic lymphohistiocytosis: An unusual complication in disseminated Mycobacterium tuberculosis
Abstract
Background: Hemophagocytic lymphohistiocytosis (HLH) is an uncommon, potentially fatal, hyperinflammatory syndrome that may rarely complicate the clinical course of disseminated Mycobacterium tuberculosis (MTB). The clinical course of tuberculosis-associated HLH (TB-HLH) has been reported to be unpredictable.
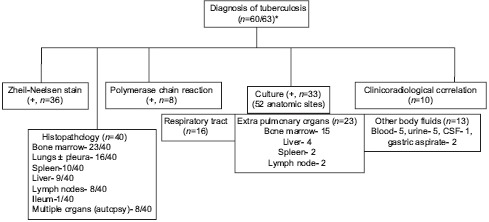
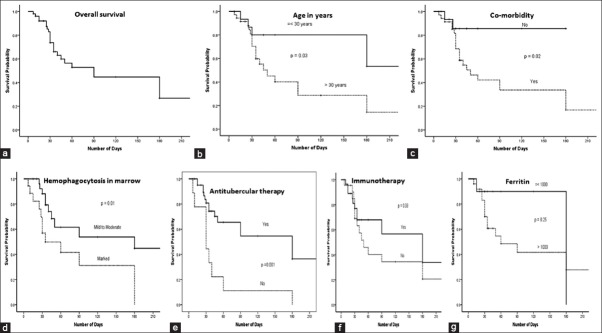
Materials and methods: Here we describe the clinicopathological features, laboratory parameters, management, and outcome data of a patient who satisfied the 2004 diagnostic criteria for HLH secondary to disseminated MTB; we also do a systematic review of the international literature on TB-HLH. The literature review (January 1975-March 2014) found that HLH complicated the clinical course of 63 tuberculosis patients (41 males, 22 females, mean age = 45 ± 23.5 years) with a high mortality rate of 49% (31/63 died). The mean serum ferritin level (n = 44/63) was 5963 ng/mL (range 500-38,539 ng/mL); and a higher proportion (54.2%) of patients had pancytopenia at presentation. On univariate analysis (n = 53/63), age >30 years [hazard ratio (HR): 2.79, 95% confidence interval (CI):1.03-7.56, P = 0.03], presence of comorbidities (HR 4.59, CI: 1.08-19.52, P = 0.04), marked hemophagocytosis in bone marrow (HR: 2.65, CI: 1.16-6.05, P = 0.02), and nonusage/delayed usage of antitubercular therapy (ATT) (HR: 3.44, CI: 1.51-7.87, P = 0.003) were associated with decreased survival, though none of these parameters attained statistical significance (P > 0.05) in multivariate analysis. Usage of corticosteroids and/or immunomodulator drugs (HR 1.00, CI: 0.66-3.22, P = 0.35) did not alter the outcome in these patients.
Conclusion: HLH should be considered as a differential diagnosis in patients with tuberculosis who present with cytopenias, organomegaly, and coagulopathy. Strong clinical suspicion and early usage of ATT might be useful in reducing the morbidity and mortality. The utility of immunosuppressive/immunomodulator therapy lacks general concensus among treating physicians, and warrants further studies.
Keywords: Antitubercular therapy; hemophagocytic lymphohistiocytosis; survival; tuberculosis.
Conflict of interest statement
Figures
References
-
- Rosado FG, Kim AS. Hemophagocytic lymphocytosis: An update on diagnosis and pathogenesis. Am J Clin Pathol. 2013;139:713–27. - PubMed
-
- Gupta S, Weitzman S. Primary and secondary hemophagocytic lymphohistiocytosis: Clinical features, pathogenesis and therapy. Expert Rev Clin Immunol. 2010;6:137–54. - PubMed
-
- Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48:124–31. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
