

Balloon Angioplasty - The Legacy of Andreas Grüntzig, M.D. (1939-1985)
- PMID: 26664865
- PMCID: PMC4671350
- DOI: 10.3389/fcvm.2014.00015
Balloon Angioplasty - The Legacy of Andreas Grüntzig, M.D. (1939-1985)
Abstract
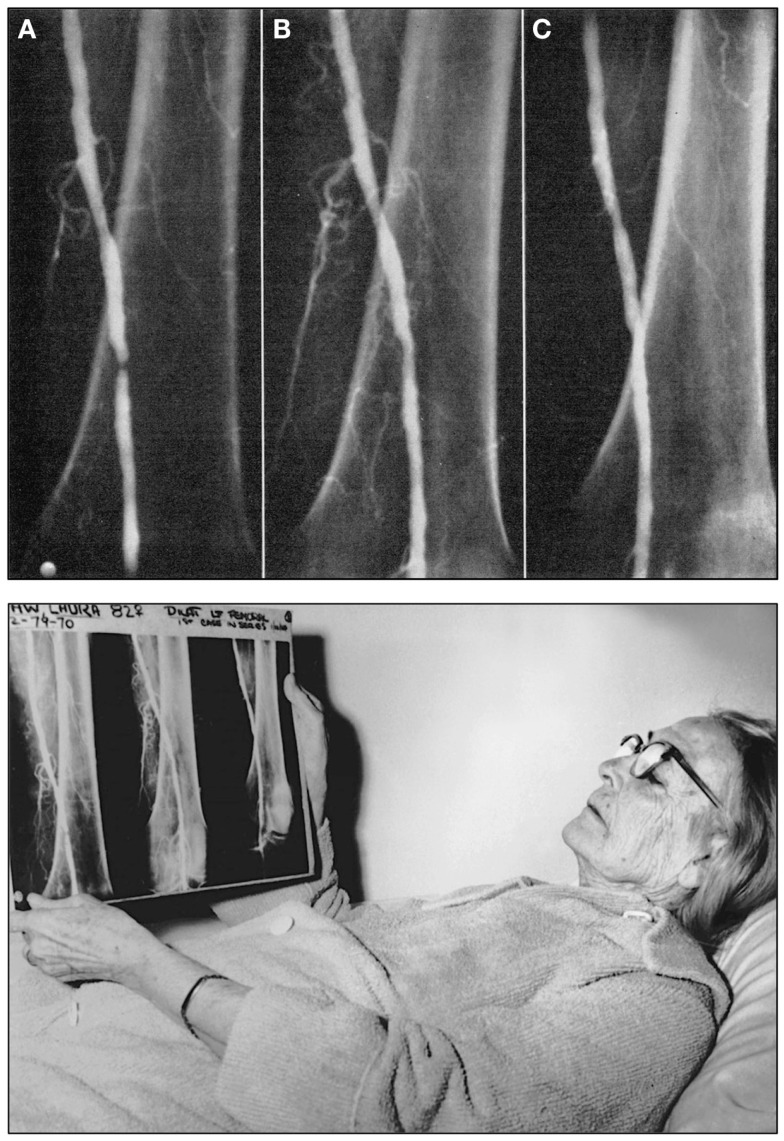
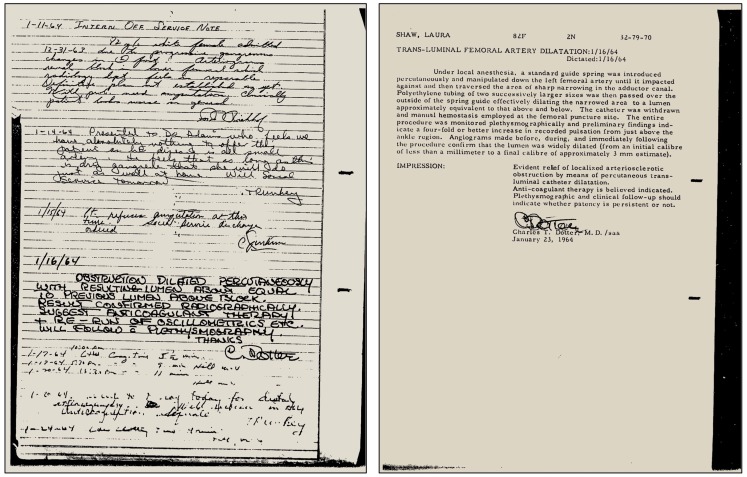
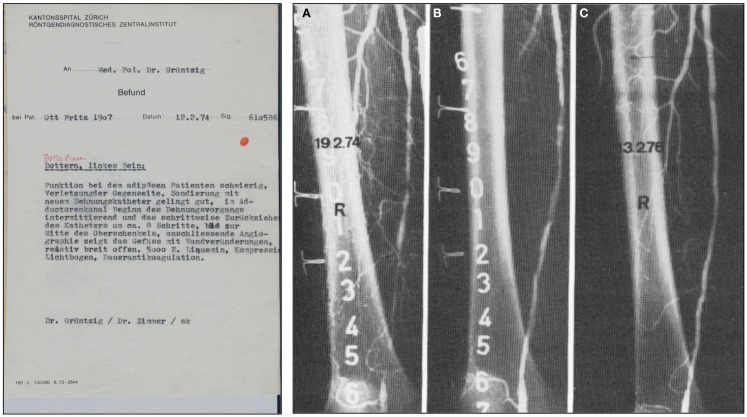
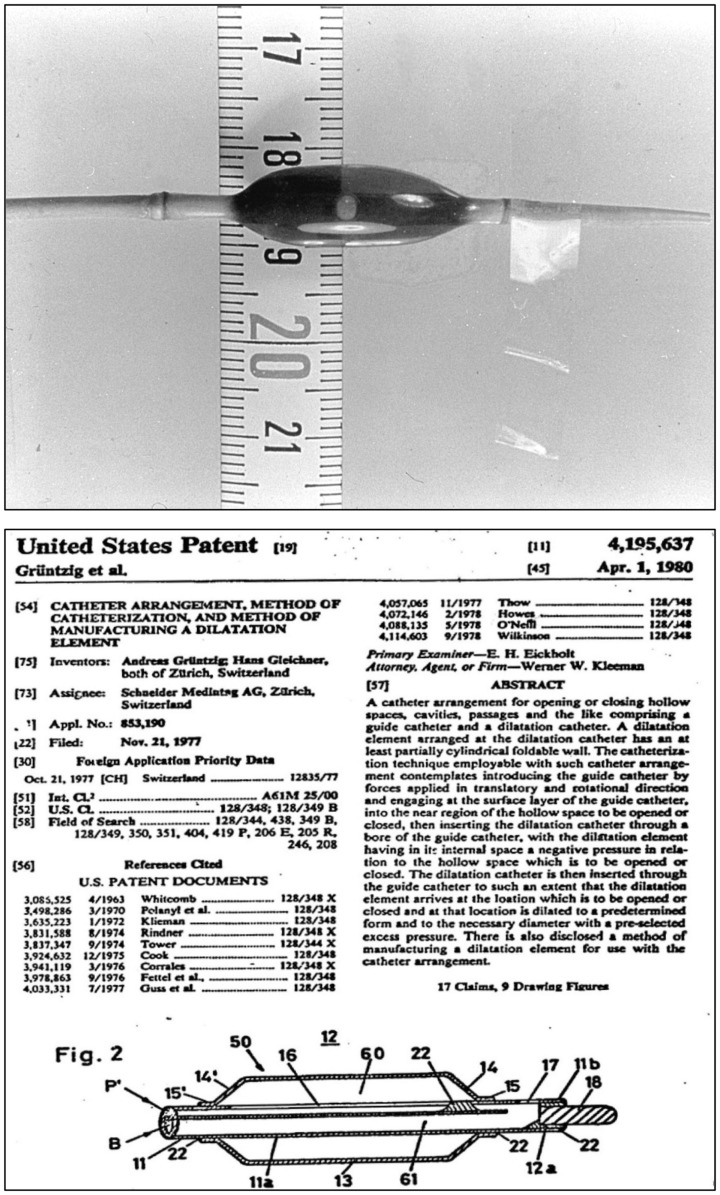
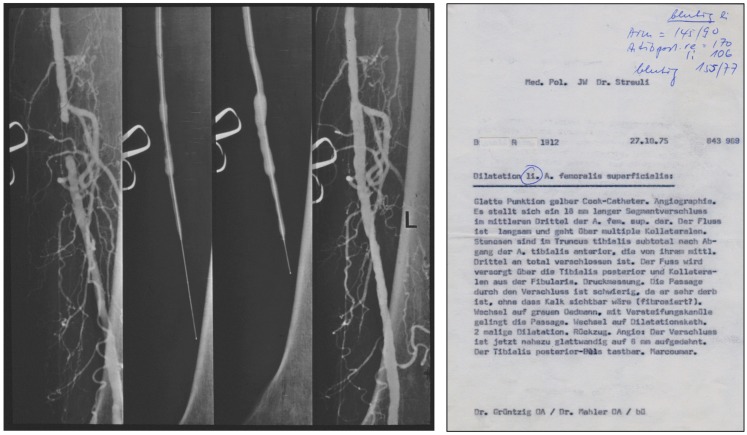
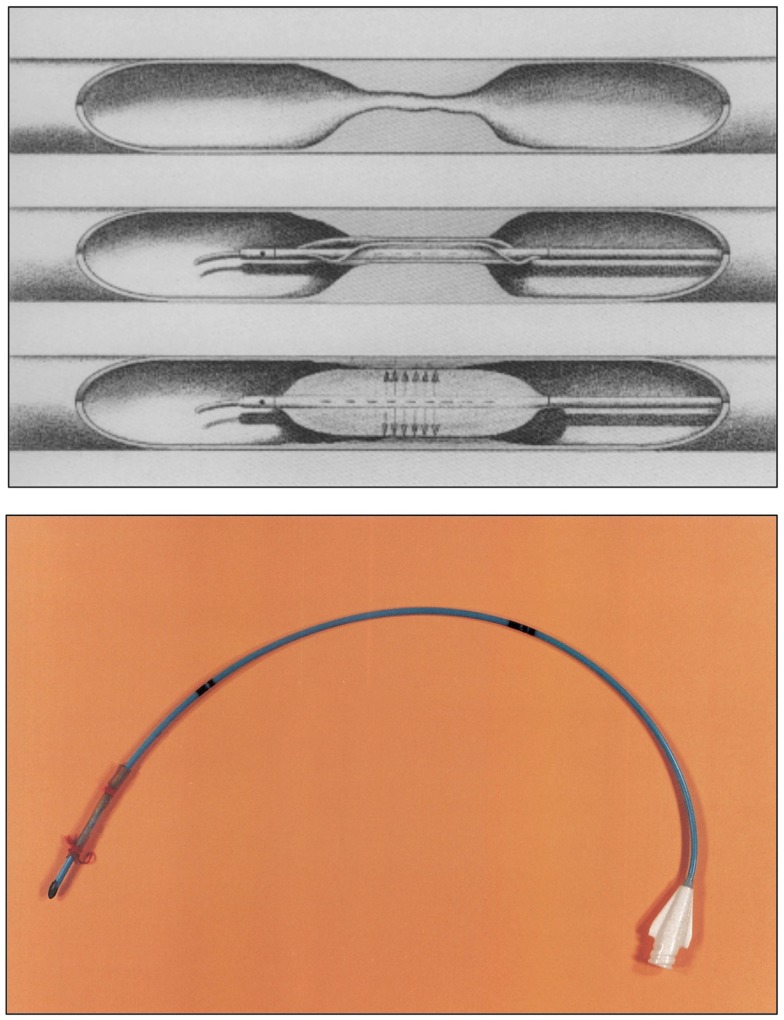
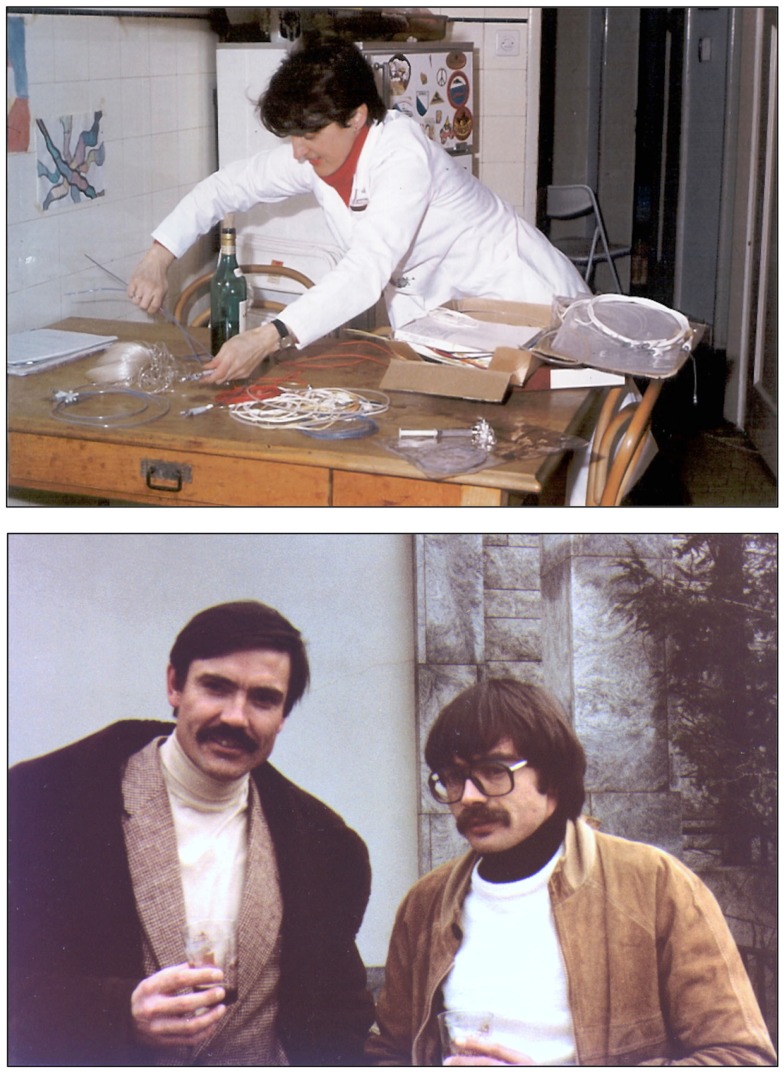
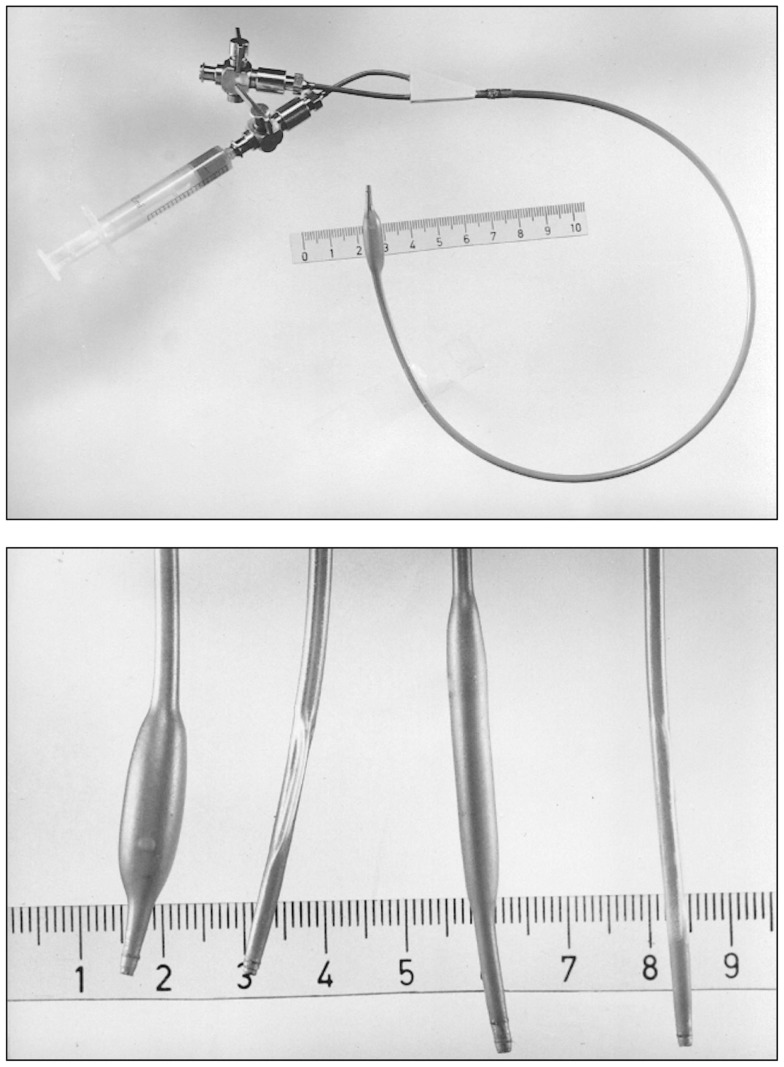
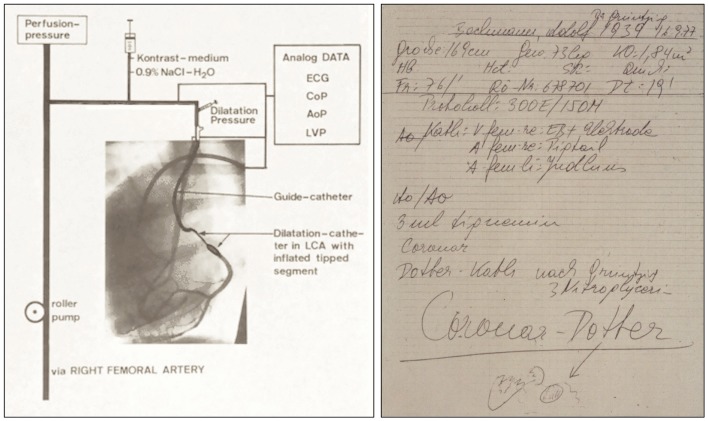
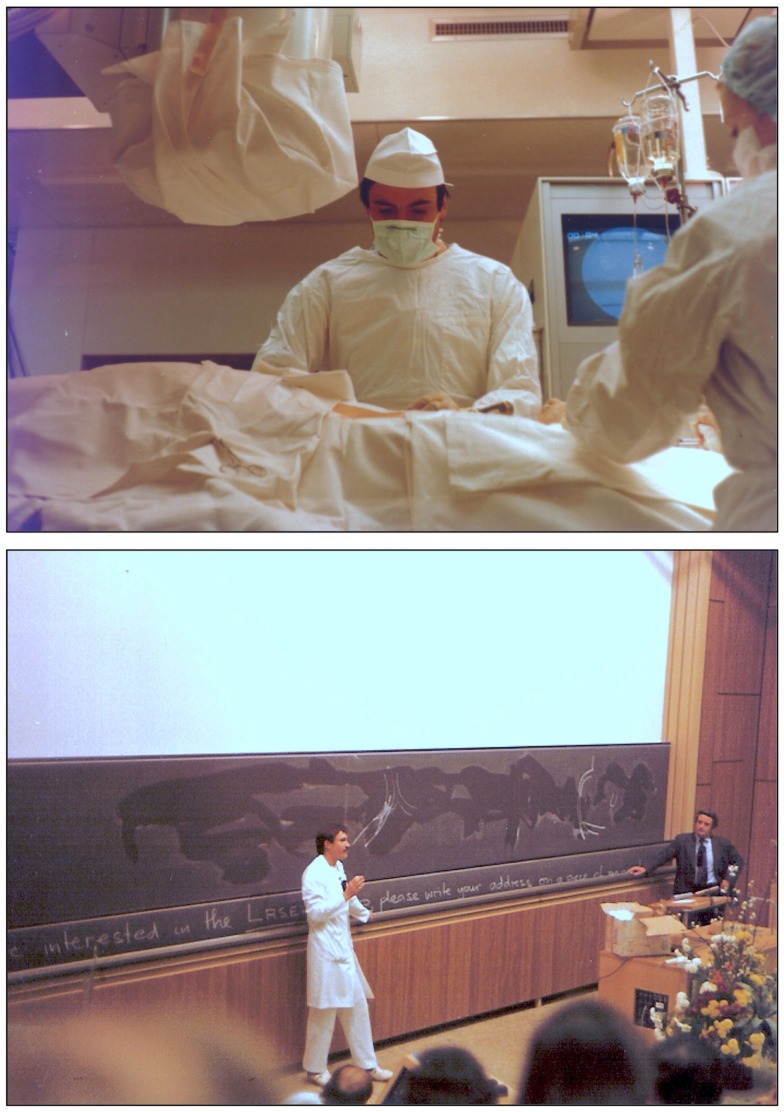
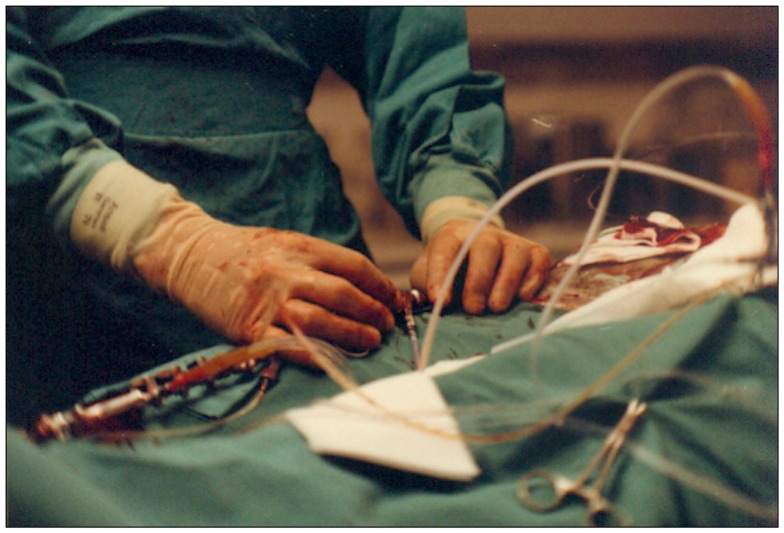
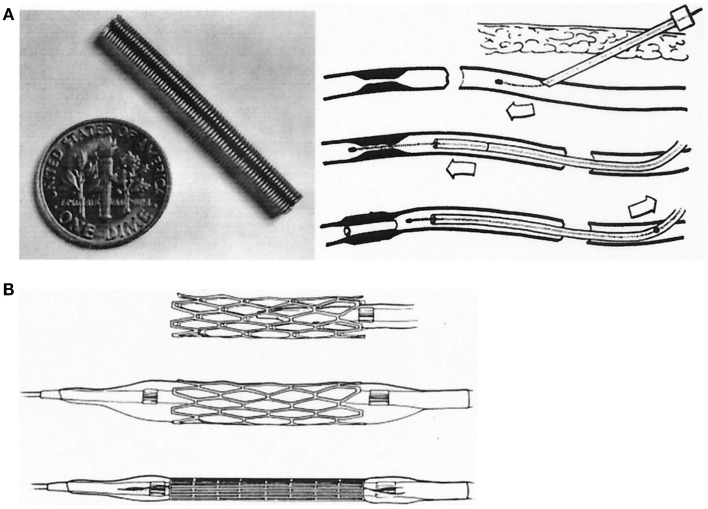
In 1974, at the Medical Policlinic of the University of Zürich, German-born physician-scientist Andreas Grüntzig (1939-1985) for the first time applied a balloon-tipped catheter to re-open a severely stenosed femoral artery, a procedure, which he initially called "percutaneous transluminal dilatation". Balloon angioplasty as a therapy of atherosclerotic vascular disease, for which Grüntzig and Charles T. Dotter (1920-1985) received a nomination for the Nobel Prize in Physiology or Medicine in 1978, became one of the most successful examples of translational medicine in the twentieth century. Known today as percutaneous transluminal angioplasty (PTA) in peripheral arteries or percutaneous transluminal coronary angioplasty (PTCA) or percutaneous coronary intervention (PCI) in coronary arteries, balloon angioplasty has become the method of choice to treat patients with acute myocardial infarction or occluded leg arteries. On the occasion of the 40(th) anniversary of balloon angioplasty, we summarize Grüntzig's life and career in Germany, Switzerland, and the United States and also review the developments in vascular medicine from the 1890s to the 1980s, including Dotter's first accidental angioplasty in 1963. The work of pioneers of catheterization, including Pedro L. Fariñas in Cuba, André F. Cournand in France, Werner Forssmann, Werner Porstmann and Eberhard Zeitler in Germany, António Egas Moniz and Reynaldo dos Santos in Portugal, Sven-Ivar Seldinger in Sweden, and Barney Brooks, Thomas J. Fogarty, Melvin P. Judkins, Richard K. Myler, Dickinson W. Richards, and F. Mason Sones in the United States, is discussed. We also present quotes by Grüntzig and excerpts from his unfinished autobiography, statements of Grüntzig's former colleagues and contemporary witnesses, and have included hitherto unpublished historic photographs and links to archive recordings and historic materials. This year, on June 25, 2014, Andreas Grüntzig would have celebrated his 75(th) birthday. This article is dedicated to his memory.
Keywords: Alexis Carrel; Andreas Gruentzig; Nobel Prize; Robert Hegglin; atherosclerosis; autobiography; biography; coronary artery disease; peripheral vascular disease.
Figures

References
-
- Grüntzig A. Ein Fragebogentest zur Diagnose der koronaren Herzkrankheit. Schweiz Rundsch Med Prax (1972) 61(34):1068–70. - PubMed
-
- Grüntzig A, Schönbeck M, Winzeler A, Lichtlen P, Rutishauser W. Die Treffsicherheit einer Fragebogendiagnose bei coronarer Herzkrankheit mit der selektiven Coronarangiographie als Referenztest. Verh Dtsch Ges Inn Med (1972) 78:1017–20. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous