

Anticoagulant Treatment of Deep Vein Thrombosis and Pulmonary Embolism: The Present State of the Art
- PMID: 26664901
- PMCID: PMC4671349
- DOI: 10.3389/fcvm.2015.00030
Anticoagulant Treatment of Deep Vein Thrombosis and Pulmonary Embolism: The Present State of the Art
Abstract
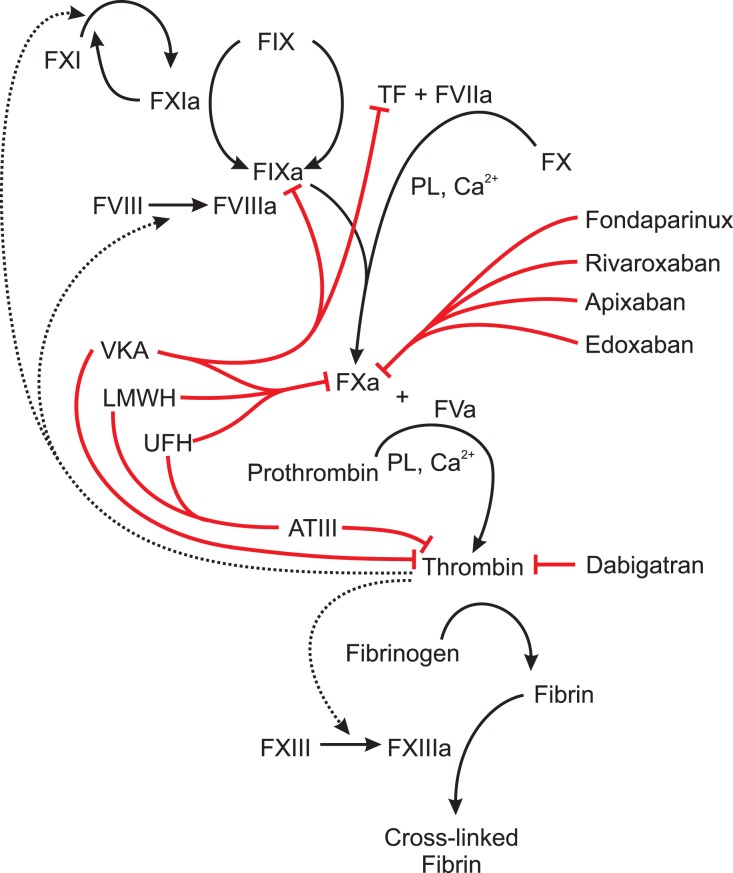
Venous thromboembolism (VTE), a disease entity comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), is a frequent and potentially life-threatening event. To date different agents are available for the effective treatment of acute VTE and the prevention of recurrence. For several years, the standard of care was the subcutaneous application of a low molecular weight heparin (LMWH) or fondaparinux, followed by a vitamin K antagonist (VKA). The so-called direct oral anticoagulants (DOAC) were introduced rather recently in clinical practice for the treatment of VTE. DOAC seem to have a favorable risk-benefit profile compared to VKA. Moreover, DOAC significantly simplify VTE treatment because they are administered in fixed doses and no routine monitoring is needed. Patients with objectively diagnosed DVT or PE should receive therapeutic anticoagulation for a minimum of 3 months. Whether a patient ought to receive extended treatment needs to be evaluated on an individual basis, depending mainly on risk factors determined by characteristics of the thrombotic event and patient-related factors. In specific patient groups (e.g., pregnant women, cancer patients, and elderly patients), treatment of VTE is more challenging than that in the general population and additional issues need to be considered in those patients. The aim of this review is to give an overview of the currently available treatment modalities of acute VTE and secondary prophylaxis. In particular, specific aspects regarding the initiation of VTE treatment, duration of anticoagulation, and specific patient groups will be discussed.
Keywords: anticoagulation; deep vein thrombosis; pulmonary embolism; secondary prevention; venous thromboembolism.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources