

Mitral Annular Kinetics, Left Atrial, and Left Ventricular Diastolic Function Post Mitral Valve Repair in Degenerative Mitral Regurgitation
- PMID: 26664902
- PMCID: PMC4671359
- DOI: 10.3389/fcvm.2015.00031
Mitral Annular Kinetics, Left Atrial, and Left Ventricular Diastolic Function Post Mitral Valve Repair in Degenerative Mitral Regurgitation
Abstract
Objective: The relationship of mitral annular (MA) kinetics to left ventricular (LV) and left atrial (LA) function before and after mitral valve (MV) repair has not been well studied. Here we sought to provide comprehensive analysis that relates to MA motions, and LA and LV diastolic function post MV repair.
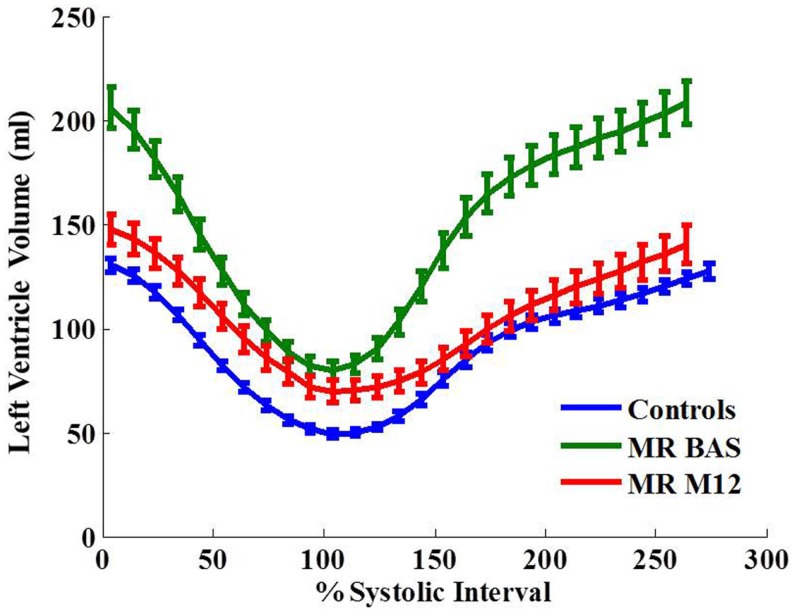
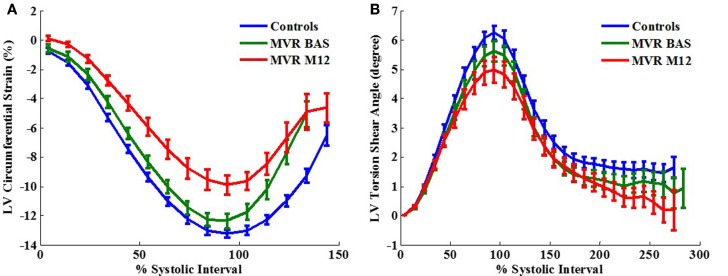
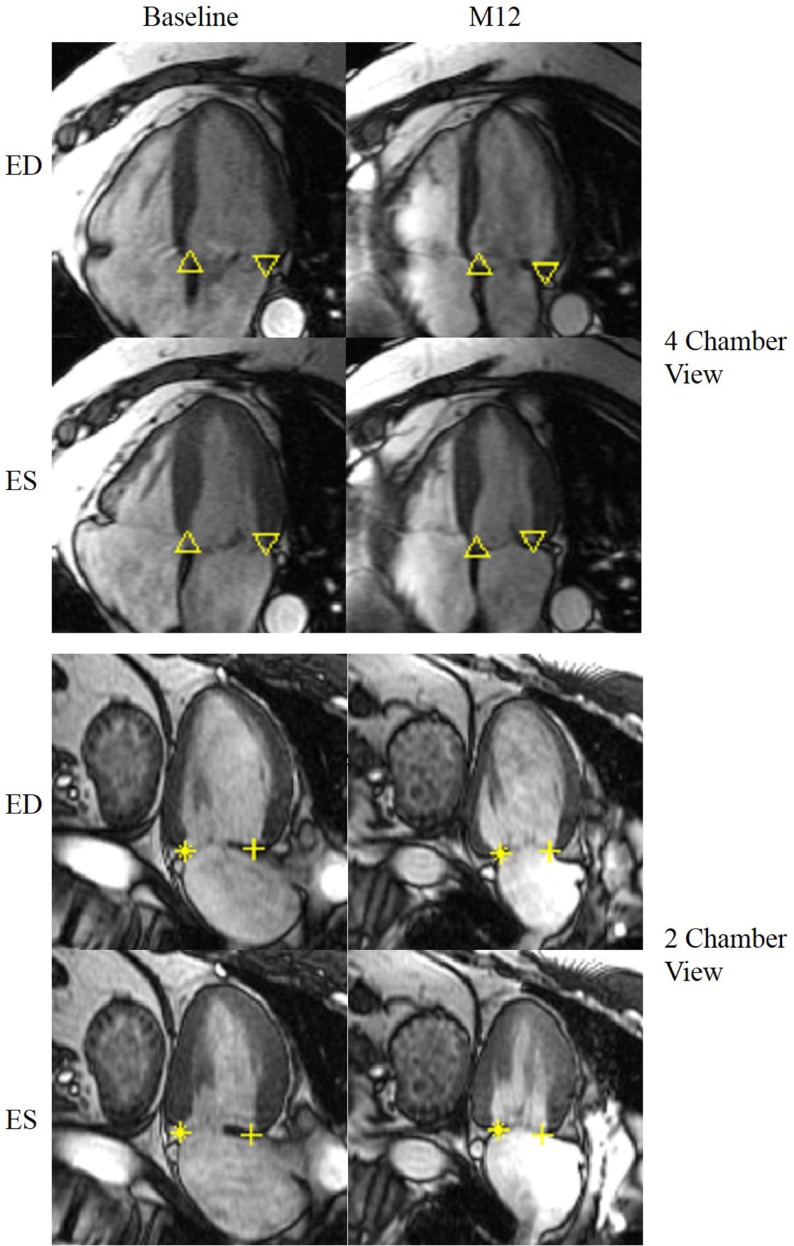
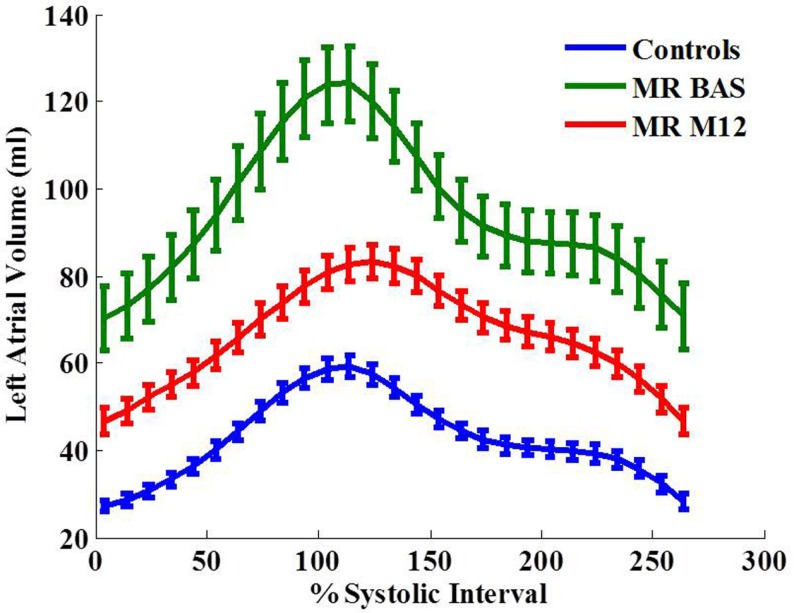
Methods: Three-dimensional analyses of mitral annular motion, LA function, and LV volumetric and diastolic strain rates were performed on 35 degenerative mitral regurgitation (MR) patients at baseline and 1-year post MV repair, and 51 normal controls, utilizing cardiac magnetic resonance imaging with tissue tagging.
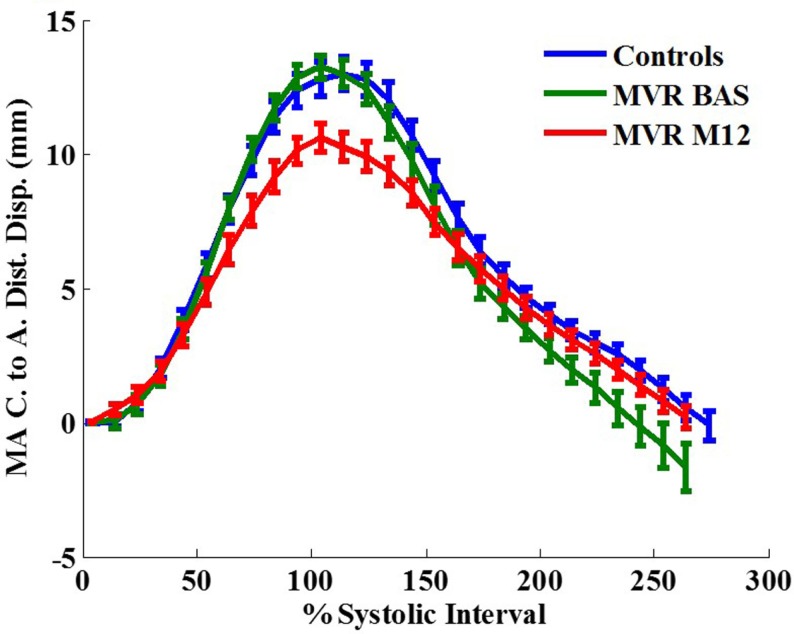
Results: All had normal LV ejection fraction (EF) at baseline. LV and LA EFs decreased 1-year post-surgery vs. controls. LV early diastolic myocardial strain rates decreased post-surgery along with decreases in normalized early diastolic filling rate, E/A ratio, and early diastolic MA relaxation rates. Post-surgical LA late active kick remained higher in MR patients vs. control. LV and LA EFs were significantly associated with peak MA centroid to apex shortening. Furthermore, during LV systolic phase, peak LV ejection and LA filling rates were significantly correlated with peak MA centroid to apex shortening rate, respectively. While during LV diastolic phase, both peak early diastolic MA centroid to apex relaxation rate and LA ejection rate were positively significantly associated with LV peak early diastolic filling rate.
Conclusion: MA motion is significantly associated with LA and LV function. Mitral annular motion, left atrial function, and LV diastolic strain rates are still impaired 1 year post MV repair. Long-term effects of these impairments should be prospectively evaluated.
Keywords: isolated mitral regurgitation; left atrial function; left ventricular diastolic function; mitral annular kinetics; mitral valve repair.
Figures
References
-
- Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr, Faxon DP, Freed MD, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol (2008) 52:e1–142.10.1016/j.jacc.2008.05.007 - DOI - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, III, Guyton RA, et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol (2014) 63:e57–185.10.1016/j.jacc.2014.02.536 - DOI - PubMed
-
- Ahmed MI, Gladden JD, Litovsky SH, Lloyd SG, Gupta H, Inusah S, et al. Increased oxidative stress and cardiomyocyte myofibrillar degeneration in patients with chronic isolated mitral regurgitation and ejection fraction >60%. J Am Coll Cardiol (2010) 55:671–9.10.1016/j.jacc.2009.08.074 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous