

US Cystic Fibrosis Foundation and European Cystic Fibrosis Society consensus recommendations for the management of non-tuberculous mycobacteria in individuals with cystic fibrosis
- PMID: 26666259
- PMCID: PMC4717371
- DOI: 10.1136/thoraxjnl-2015-207360
US Cystic Fibrosis Foundation and European Cystic Fibrosis Society consensus recommendations for the management of non-tuberculous mycobacteria in individuals with cystic fibrosis
Abstract
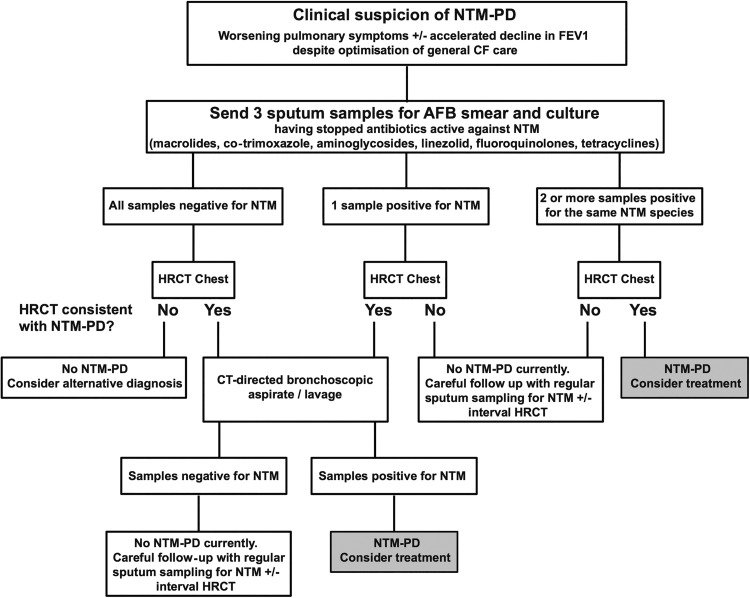
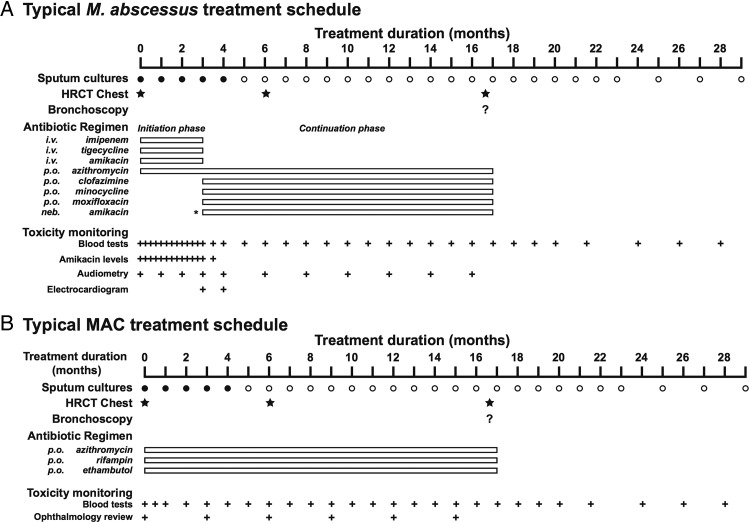
Non-tuberculous mycobacteria (NTM) are ubiquitous environmental organisms that can cause chronic pulmonary infection, particularly in individuals with pre-existing inflammatory lung disease such as cystic fibrosis (CF). Pulmonary disease caused by NTM has emerged as a major threat to the health of individuals with CF but remains difficult to diagnose and problematic to treat. In response to this challenge, the US Cystic Fibrosis Foundation (CFF) and the European Cystic Fibrosis Society (ECFS) convened an expert panel of specialists to develop consensus recommendations for the screening, investigation, diagnosis and management of NTM pulmonary disease in individuals with CF. Nineteen experts were invited to participate in the recommendation development process. Population, Intervention, Comparison, Outcome (PICO) methodology and systematic literature reviews were employed to inform draft recommendations. An anonymous voting process was used by the committee to reach consensus. All committee members were asked to rate each statement on a scale of: 0, completely disagree, to 9, completely agree; with 80% or more of scores between 7 and 9 being considered 'good' agreement. Additionally, the committee solicited feedback from the CF communities in the USA and Europe and considered the feedback in the development of the final recommendation statements. Three rounds of voting were conducted to achieve 80% consensus for each recommendation statement. Through this process, we have generated a series of pragmatic, evidence-based recommendations for the screening, investigation, diagnosis and treatment of NTM infection in individuals with CF as an initial step in optimising management for this challenging condition.
Keywords: Bacterial Infection; Cystic Fibrosis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical