

Diabetes and Prior Coronary Heart Disease are Not Necessarily Risk Equivalent for Future Coronary Heart Disease Events
- PMID: 26666660
- PMCID: PMC4803685
- DOI: 10.1007/s11606-015-3556-3
Diabetes and Prior Coronary Heart Disease are Not Necessarily Risk Equivalent for Future Coronary Heart Disease Events
Abstract
Background: For more than a decade, the presence of diabetes has been considered a coronary heart disease (CHD) "risk equivalent".
Objective: The objective of this study was to revisit the concept of risk equivalence by comparing the risk of subsequent CHD events among individuals with or without history of diabetes or CHD in a large contemporary real-world cohort over a period of 10 years (2002 to 2011).
Design: Population-based prospective cohort analysis.
Participants: We studied a cohort of 1,586,061 adult members (ages 30-90 years) of Kaiser Permanente Northern California, an integrated health care delivery system.
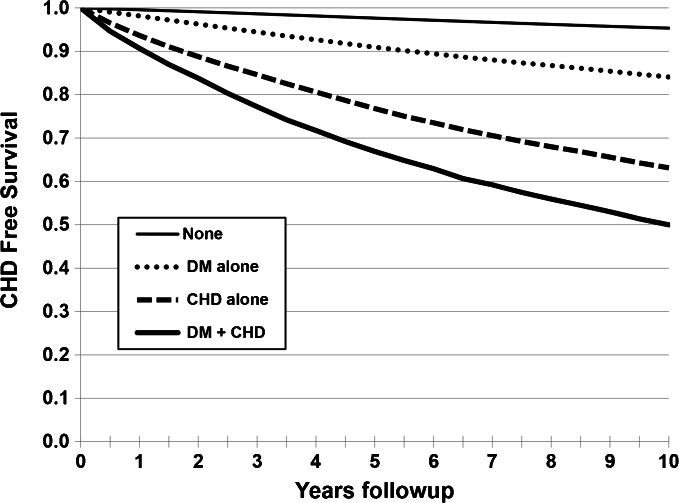
Main measurements: We calculated hazard ratios (HRs) from Cox proportional hazard models for CHD among four fixed cohorts, defined by prevalent (baseline) risk group: no history of diabetes or CHD (None), prior CHD alone (CHD), diabetes alone (DM), and diabetes and prior CHD (DM + CHD).
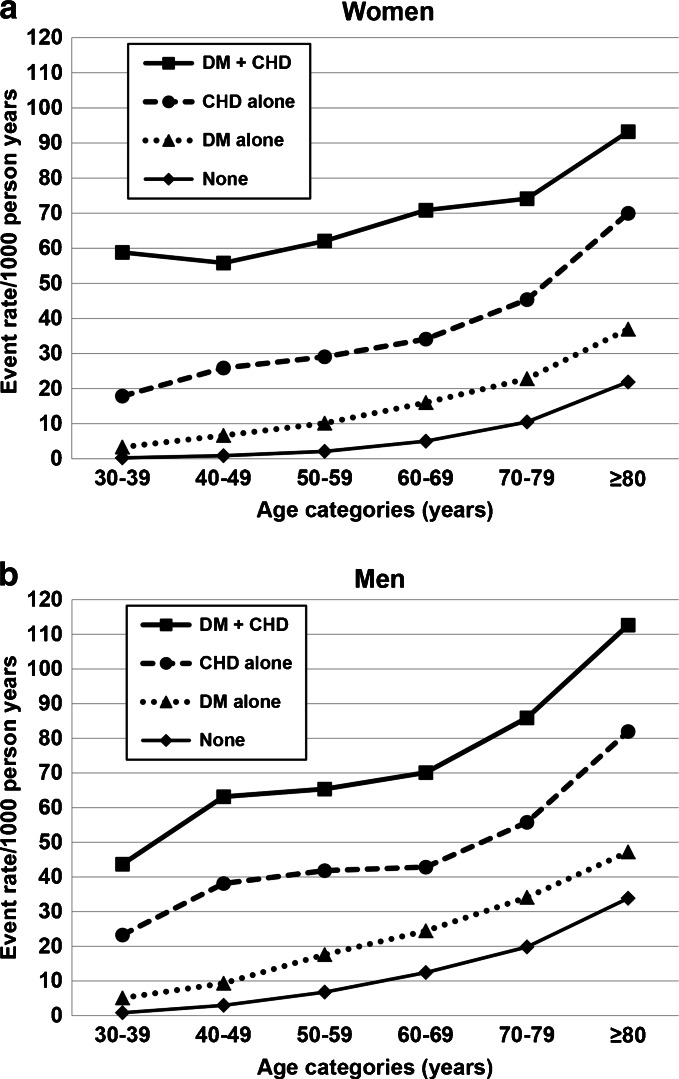
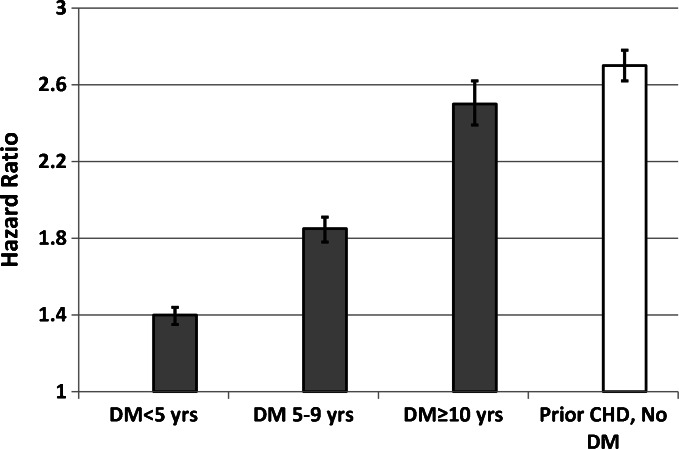
Key results: We observed 80,012 new CHD events over the follow-up period (~10,980,800 person-years). After multivariable adjustment, the HRs (reference: None) for new CHD events were as follows: CHD alone, 2.8 (95% CI, 2.7-2.85); DM alone 1.7 (95% CI, 1.66-1.74); DM + CHD, 3.9 (95% CI, 3.8-4.0). Individuals with diabetes alone had significantly lower risk of CHD across all age and sex strata compared to those with CHD alone (12.2 versus 22.5 per 1000 person-years). The risk of future CHD for patients with a history of either DM or CHD was similar only among those with diabetes of long duration (≥10 years).
Conclusions: Not all individuals with diabetes should be unconditionally assumed to be a risk equivalent of those with prior CHD.
Keywords: coronary heart disease; diabetes; epidemiology.
Conflict of interest statement
Compliance with Ethical Standards Funding Sources This study was supported by a grant from the Kaiser Permanente Northern California Community Benefit Program. Conflict of Interest The authors declare no conflicts of interest.
Figures
Comment in
-
Capsule Commentary on Rana et al., Diabetes and Prior Coronary Heart Disease Are Not Necessarily Risk Equivalent for Future Coronary Heart Disease Events.J Gen Intern Med. 2016 Apr;31(4):413. doi: 10.1007/s11606-016-3605-6. J Gen Intern Med. 2016. PMID: 26873149 Free PMC article. No abstract available.
References
-
- Executive summary of the third report of the national cholesterol education program (NCEP) Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001; 285: 2486–97. - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Sr, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC, Jr, Sorlie P, Stone NJ, Wilson PW, American College of Cardiology/American Heart Association Task Force on Practice Guidelines ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American college of cardiology/American heart association task force on practice guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2935–2959. doi: 10.1016/j.jacc.2013.11.005. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
