

Does Critical Illness Change Levofloxacin Pharmacokinetics?
- PMID: 26666946
- PMCID: PMC4775952
- DOI: 10.1128/AAC.02610-15
Does Critical Illness Change Levofloxacin Pharmacokinetics?
Abstract
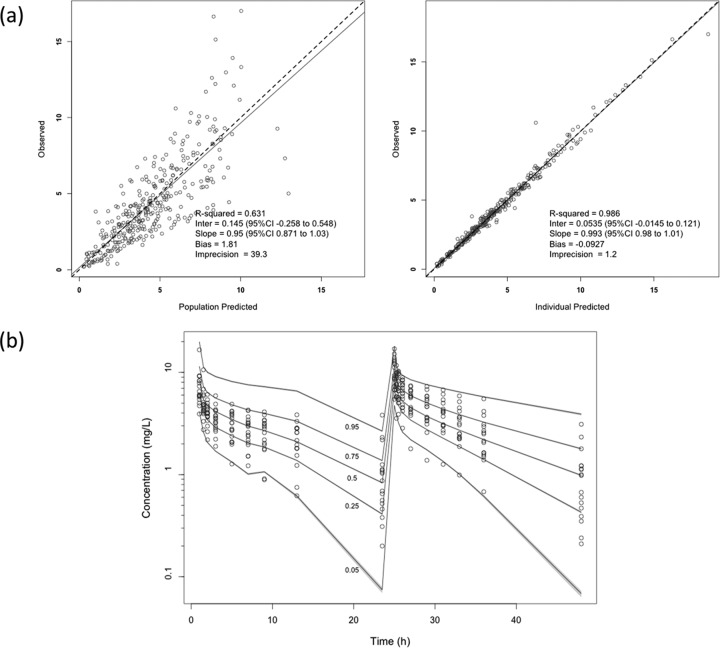
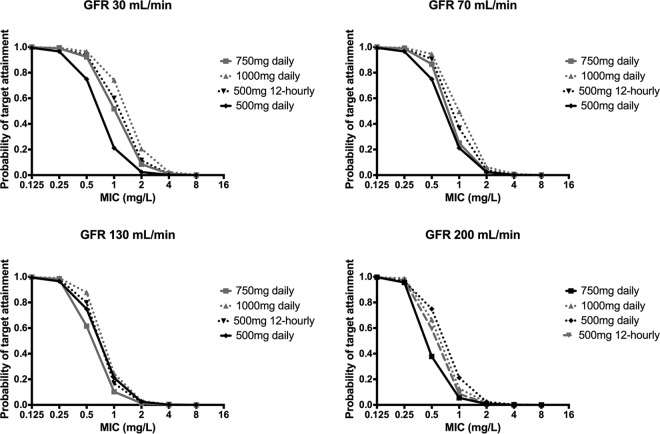
Levofloxacin is commonly used in critically ill patients for which existing data suggest nonstandard dosing regimens should be used. The objective of this study was to compare the population pharmacokinetics of levofloxacin in critically ill and in non-critically ill patients. Adult patients with a clinical indication for levofloxacin were eligible for participation in this prospective pharmacokinetic study. Patients were given 500 mg or 750 mg daily by intravenous administration with up to 11 blood samples taken on day 1 or 2 of therapy. Plasma samples were analyzed and population pharmacokinetic analysis was undertaken using Pmetrics. Thirty-five patients (18 critically ill) were included. The mean (standard deviation [SD]) age, weight, and Cockcroft-Gault creatinine clearance for the critically ill and for the non-critically ill patients were 60.3 (16.4) and 72.0 (11.6) years, 78.5 (14.8) and 70.9 (15.8) kg, and 71.9 (65.8) and 68.2 (30.1) ml/min, respectively. A two-compartment linear model best described the data. Increasing creatinine clearance was the only covariate associated with increasing drug clearance. The presence of critical illness did not significantly affect any pharmacokinetic parameter. The mean (SD) parameter estimates were as follows: clearance, 8.66 (3.85) liters/h; volume of the central compartment (Vc), 41.5 (24.5) liters; intercompartmental clearance constants from central to peripheral, 2.58 (3.51) liters/h; and peripheral to central compartments, 0.90 (0.58) liters/h. Monte Carlo dosing simulations demonstrated that achievement of therapeutic exposures was dependent on renal function, pathogen, and MIC. Critical illness appears to have no independent effect on levofloxacin pharmacokinetics that cannot be explained by altered renal function.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Boselli E, Breilh D, Rimmele T, Djabarouti S, Saux MC, Chassard D, Allaouchiche B. 2005. Pharmacokinetics and intrapulmonary diffusion of levofloxacin in critically ill patients with severe community-acquired pneumonia. Crit Care Med 33:104–109. doi:10.1097/01.CCM.0000150265.42067.4C. - DOI - PubMed
-
- Furlanut M, Brollo L, Lugatti E, Di Qual E, Dolcet F, Talmassons G, Pea F. 2003. Pharmacokinetic aspects of levofloxacin 500 mg once daily during sequential intravenous/oral therapy in patients with lower respiratory tract infections. J Antimicrob Chemother 51:101–106. doi:10.1093/jac/dkg035. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
