

Associations of Left Ventricular Hypertrophy and Geometry with Adverse Outcomes in Patients with CKD and Hypertension
- PMID: 26668021
- PMCID: PMC4741044
- DOI: 10.2215/CJN.06980615
Associations of Left Ventricular Hypertrophy and Geometry with Adverse Outcomes in Patients with CKD and Hypertension
Abstract
Background and objectives: Left ventricular hypertrophy (LVH) and abnormal left ventricular (LV) geometry predict adverse outcomes in the general and hypertensive populations, but findings in CKD are still inconclusive.
Design, setting, participants, & measurements: We enrolled 445 patients with hypertension and CKD stages 2-5 in two academic nephrology clinics in 1999-2003 who underwent both echocardiography and ambulatory BP monitoring. LVH (LV mass >100 g/m(2) [women] and >131 g/m(2) [men]) and relative wall thickness (RWT) were used to define LV geometry: no LVH and RWT≤0.45 (normal), no LVH and RWT>0.45 (remodeling), LVH and RWT≤0.45 (eccentric), and LVH and RWT>0.45 (concentric). We evaluated the prognostic role of LVH and LV geometry on cardiovascular (CV; composite of fatal and nonfatal events) and renal outcomes (composite of ESRD and all-cause death).
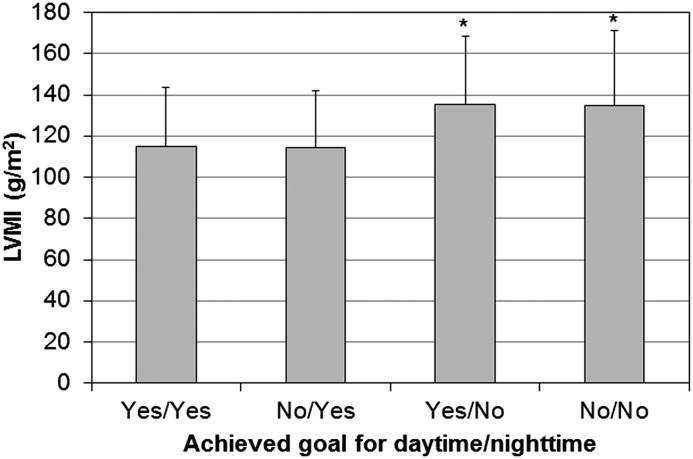
Results: Age was 64.1±13.8 years old; 19% had diabetes, and 22% had CV disease. eGFR was 39.9±20.2 ml/min per 1.73 m(2). LVH was detected in 249 patients (56.0%); of these, 125 had concentric LVH, and 124 had eccentric pattern, whereas 71 patients had concentric remodeling. Age, women, anemia, and nocturnal hypertension were independently associated with both concentric and eccentric LVH, whereas diabetes and history of CV disease associated with eccentric LVH only, and CKD stages 4 and 5 associated with concentric LVH only. During follow-up (median, 5.9 years; range, 0.04-15.3), 188 renal deaths (112 ESRD) and 103 CV events (61 fatal) occurred. Using multivariable Cox analysis, concentric and eccentric LVH was associated with higher risk of CV outcomes (hazard ratio [HR], 2.59; 95% confidence interval [95% CI], 1.39 to 4.84 and HR, 2.79; 95% CI, 1.47 to 5.26, respectively). Similarly, greater risk of renal end point was detected in concentric (HR, 2.33; 95% CI, 1.44 to 3.80) and eccentric (HR, 2.30; 95% CI, 1.42 to 3.74) LVH. Sensitivity analysis using LVH and RWT separately showed that LVH but not RWT was associated with higher cardiorenal risk.
Conclusions: In patients with CKD, LVH is a strong predictor of the risk of poor CV and renal outcomes independent from LV geometry.
Keywords: blood pressure monitoring, ambulatory; chronic kidney disease; echocardiography; female; follow-up studies; humans; hypertension; hypertrophy, left ventricular; left ventricular geometry.
Copyright © 2016 by the American Society of Nephrology.
Figures



References
-
- Paoletti E, Bellino D, Cassottana P, Rolla D, Cannella G: Left ventricular hypertrophy in nondiabetic predialysis CKD. Am J Kidney Dis 46: 320–327, 2005 - PubMed
-
- De Nicola L, Minutolo R, Chiodini P, Zoccali C, Castellino P, Donadio C, Strippoli M, Casino F, Giannattasio M, Petrarulo F, Virgilio M, Laraia E, Di Iorio BR, Savica V, Conte G, TArget Blood Pressure LEvels in Chronic Kidney Disease (TABLE in CKD) Study Group : Global approach to cardiovascular risk in chronic kidney disease: Reality and opportunities for intervention. Kidney Int 69: 538–545, 2006 - PubMed
-
- Levin A, Singer J, Thompson CR, Ross H, Lewis M: Prevalent left ventricular hypertrophy in the predialysis population: Identifying opportunities for intervention. Am J Kidney Dis 27: 347–354, 1996 - PubMed
-
- Park M, Hsu CY, Li Y, Mishra RK, Keane M, Rosas SE, Dries D, Xie D, Chen J, He J, Anderson A, Go AS, Shlipak MG, Chronic Renal Insufficiency Cohort (CRIC) Study Group : Associations between kidney function and subclinical cardiac abnormalities in CKD. J Am Soc Nephrol 23: 1725–1734, 2012 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
