

Predictors of Subclinical Atheromatosis Progression over 2 Years in Patients with Different Stages of CKD
- PMID: 26668022
- PMCID: PMC4741032
- DOI: 10.2215/CJN.01240215
Predictors of Subclinical Atheromatosis Progression over 2 Years in Patients with Different Stages of CKD
Abstract
Background and objectives: Ultrasonographic detection of subclinical atheromatosis is a noninvasive method predicting cardiovascular events. Risk factors predicting atheromatosis progression in CKD are unknown. Predictors of atheromatosis progression were evaluated in patients with CKD.
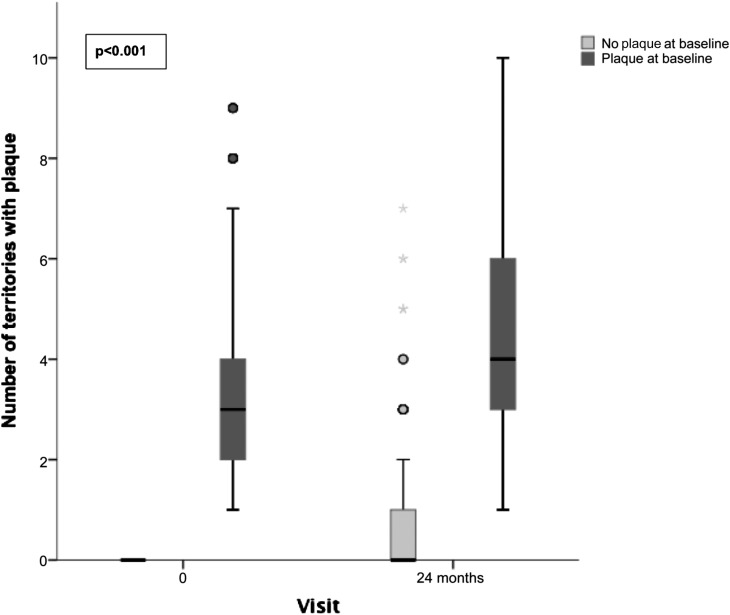
Design, setting, participants, & measurements: Our multicenter, prospective, observational study included 1553 patients with CKD (2009-2011). Carotid and femoral ultrasounds were performed at baseline and after 24 months. A subgroup of 476 patients with CKD was also randomized to undergo ultrasound examination at 12 months. Progression of atheromatosis was defined as an increase in the number of plaque territories analyzed by multivariate logistic regression.
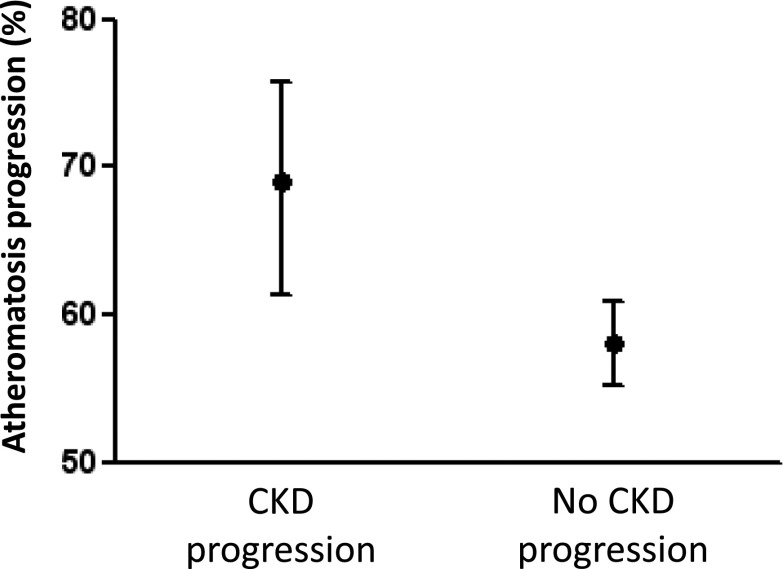
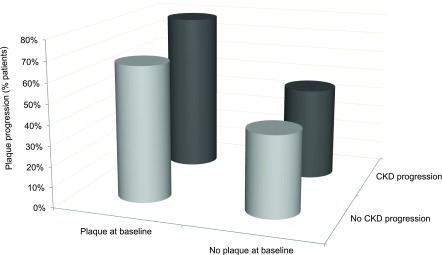
Results: Prevalence of atheromatosis was 68.7% and progressed in 59.8% of patients after 24 months. CKD progression was associated with atheromatosis progression, suggesting a close association between pathologies. Variables significantly predicting atheromatosis progression, independent from CKD stages, were diabetes and two interactions of age with ferritin and plaque at baseline. Given that multiple interactions were found between CKD stage and age, phosphate, smoking, dyslipidemia, body mass index, systolic BP (SBP), carotid intima-media thickness, plaque at baseline, uric acid, cholesterol, 25-hydroxy vitamin D (25OH vitamin D), and antiplatelet and phosphate binders use, the analysis was stratified by CKD stages. In stage 3, two interactions (age with phosphate and plaque at baseline) were found, and smoking, diabetes, SBP, low levels of 25OH vitamin D, and no treatment with phosphate binders were positively associated with atheromatosis progression. In stages 4 and 5, three interactions (age with ferritin and plaque and plaque with smoking) were found, and SBP was positively associated with atheromatosis progression. In dialysis, an interaction between body mass index and 25OH vitamin D was found, and age, dyslipidemia, carotid intima-media thickness, low cholesterol, ferritin, and uric acid were positively associated with atheromatosis progression.
Conclusions: Atheromatosis progression affects more than one half of patients with CKD, and predictive factors differ depending on CKD stage.
Keywords: atherosclerosis; blood pressure; cardiovascular disease; carotid intima-media thickness; chronic kidney disease; follow-up studies; humans; renal insufficiency, chronic; smoking; vitamin D.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Chang A, Kramer H: Should eGFR and albuminuria be added to the Framingham risk score? Chronic kidney disease and cardiovascular disease risk prediction. Nephron Clin Pract 119: c171–c177, 2011 - PubMed
-
- Coll B, Betriu A, Martínez-Alonso M, Borràs M, Craver L, Amoedo ML, Marco MP, Sarró F, Junyent M, Valdivielso JM, Fernández E: Cardiovascular risk factors underestimate atherosclerotic burden in chronic kidney disease: Usefulness of non-invasive tests in cardiovascular assessment. Nephrol Dial Transplant 25: 3017–3025, 2010 - PubMed
-
- Weiner DE, Tighiouart H, Griffith JL, Elsayed E, Levey AS, Salem DN, Sarnak MJ: Kidney disease, Framingham risk scores, and cardiac and mortality outcomes. Am J Med 120: 552.e1–552.e8, 2007 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
