

Epidemiology of Kidney Discard from Expanded Criteria Donors Undergoing Donation after Circulatory Death
- PMID: 26668028
- PMCID: PMC4741045
- DOI: 10.2215/CJN.07190715
Epidemiology of Kidney Discard from Expanded Criteria Donors Undergoing Donation after Circulatory Death
Abstract
Background and objectives: The broader use of combined expanded criteria donor and donation after circulatory death (ECD/DCD) kidneys may help expand the deceased donor pool. The purpose of our study was to evaluate discard rates of kidneys from ECD/DCD donors and factors associated with discard.
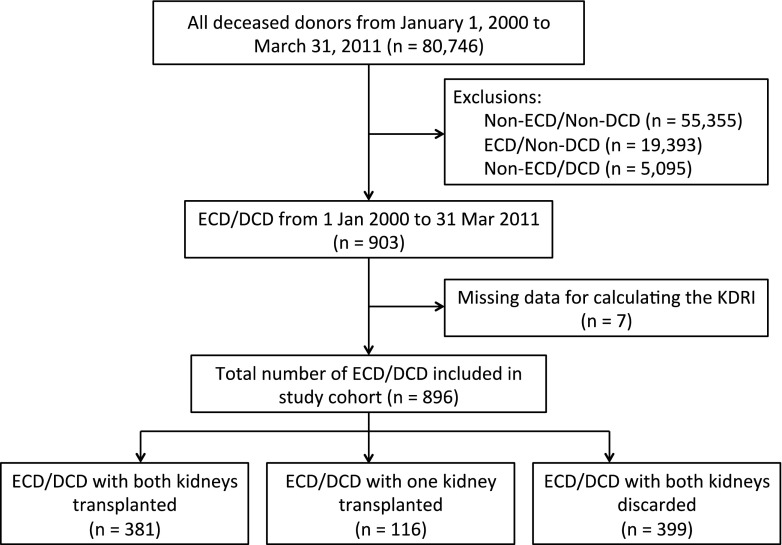
Design, setting, participants, & measurements: ECD/DCD donors and kidneys were evaluated from January 1, 2000 to March 31, 2011 using data from the Scientific Registry of Transplant Recipients. The kidney donor risk index was calculated for all ECD/DCD kidneys. Multivariable logistic regression models were used to determine risk factors for discarding both donor kidneys. The Kaplan-Meier product limit method and the log-rank statistic were used to assess the cumulative probability of graft failure for transplants from ECD/DCD donors where the mate kidney was discarded versus both kidneys were used.
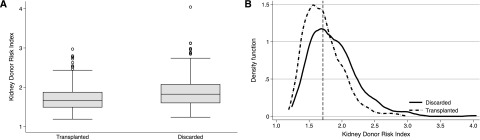
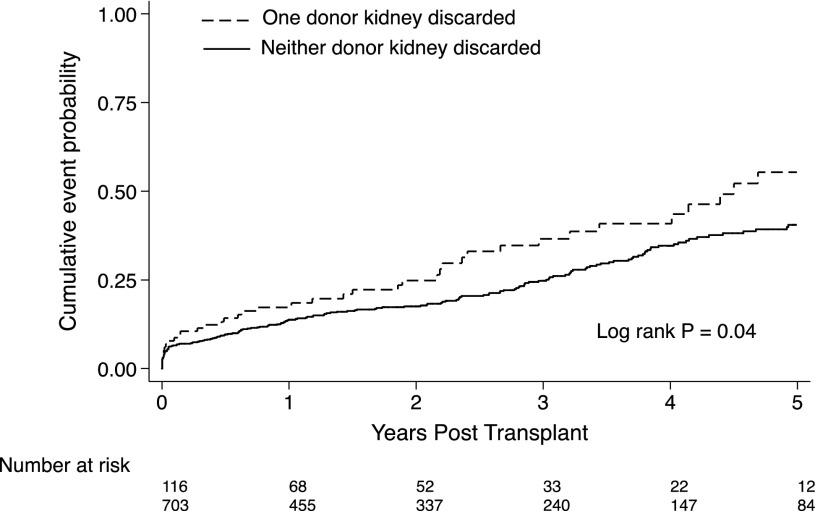
Results: There were 896 ECD/DCD donors comprising 1792 kidneys. Both kidneys were discarded in 44.5% of donors, whereas 51.0% of all available kidneys were discarded. The kidney donor risk index scores were higher among donors of discarded versus transplanted kidneys (median, 1.82; interquartile range, 1.60, 2.07 versus median, 1.67; interquartile range, 1.49, 1.87, respectively; P<0.001); however, the distributions showed considerable overlap. The adjusted odds ratios for discard were higher among donors who were older, diabetic, AB blood type, and hepatitis C positive. The cumulative probabilities of total graft failure at 1, 3, and 5 years were 17.3%, 36.5%, and 55.4% versus 13.8%, 24.7%, and 40.5% among kidneys from donors where only one versus both kidneys were transplanted, respectively (log rank P=0.04).
Conclusions: Our study shows a significantly higher discard rate for ECD/DCD kidneys versus prior reports. Some discarded ECD/DCD kidneys may be acceptable for transplantation. Additional studies are needed to evaluate the factors that influence decision making around the use of ECD/DCD kidneys.
Keywords: cadaver organ transplantation; donation after circulatory death; epidemiology and outcomes; expanded criteria donor; kidney; kidney transplantation; registries; risk factors; tissue donors; transplant recipients.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C, Muirhead N: A study of the quality of life and cost-utility of renal transplantation. Kidney Int 50: 235–242, 1996 - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- US Renal Data System: Annual Data Report: Atlas of End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2013
-
- Canadian Institute for Health Information : Canadian Organ Replacement Register Annual Report. Treatment of End-Stage Organ Failure in Canada, Ottawa, ON, Canada, Canadian Institute of Health Sciences, 2011
-
- Snoeijs MG, Winkens B, Heemskerk MB, Hoitsma AJ, Christiaans MH, Buurman WA, van Heurn LW: Kidney transplantation from donors after cardiac death: A 25-year experience. Transplantation 90: 1106–1112, 2010 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
