

Updated experiences with minimally invasive McKeown esophagectomy for esophageal cancer
- PMID: 26668512
- PMCID: PMC4671043
- DOI: 10.3748/wjg.v21.i45.12873
Updated experiences with minimally invasive McKeown esophagectomy for esophageal cancer
Abstract
Aim: To update our experiences with minimally invasive McKeown esophagectomy for esophageal cancer.
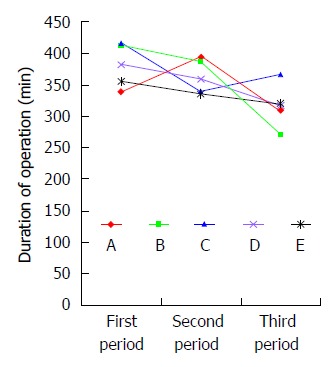
Methods: We retrospectively reviewed the medical records of 445 consecutive patients who underwent minimally invasive McKeown esophagectomy between January 2009 and July 2015 at the Cancer Hospital of Chinese Academy of Medical Sciences and used 103 patients who underwent open McKeown esophagectomy in the same period as controls. Among 375 patients who underwent total minimally invasive McKeown esophagectomy, 180 in the early period were chosen for the study of learning curve of total minimally invasive McKeown esophagectomy. These 180 minimally invasive McKeown esophagectomies performed by five surgeons were divided into three groups according to time sequence as group 1 (n = 60), group 2 (n = 60) and group 3 (n = 60).
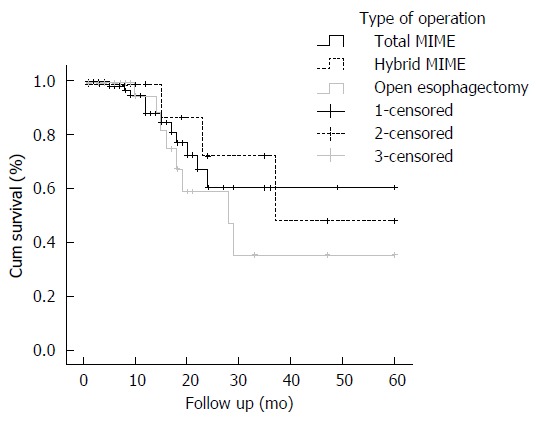
Results: Patients who underwent total minimally invasive McKeown esophagectomy had significantly less intraoperative blood loss than patients who underwent hybrid minimally invasive McKeown esophagectomy or open McKeown esophagectomy (100 mL vs 300 mL vs 200 mL, P = 0.001). However, there were no significant differences in operation time, number of harvested lymph nodes, or postoperative morbidity including incidence of pulmonary complication and anastomotic leak between total minimally invasive McKeown esophagectomy, hybrid minimally invasive McKeown esophagectomy and open McKeown esophagectomy groups. There were no significant differences in 5-year survival between these three groups (60.5% vs 47.9% vs 35.6%, P = 0.735). Patients in group 1 had significantly longer duration of operation than those in groups 2 and 3. There were no significant differences in intraoperative blood loss, number of harvested lymph nodes, or postoperative morbidity including incidence of pulmonary complication and anastomotic leak between groups 1, 2 and 3.
Conclusion: Total minimally invasive McKeown esophagectomy was associated with reduced intraoperative blood loss and comparable short term and long term survival compared with hybrid minimally invasive McKeown esophagectomy or open Mckeown esophagectomy. At least 12 cases are needed to master total minimally invasive McKeown esophagectomy in a high volume center.
Keywords: Esophagectomy; Learning curve; Minimally invasive; Outcome; Surgical procedures.
Figures
Similar articles
-
Clinical analysis of minimally invasive McKeown esophagectomy in a single center by a single medical group.J Zhejiang Univ Sci B. 2018 Sept.;19(9):718-725. doi: 10.1631/jzus.B1800329. J Zhejiang Univ Sci B. 2018. PMID: 30178638 Free PMC article.
-
Comparative study of minimally invasive versus open esophagectomy for esophageal cancer in a single cancer center.Chin Med J (Engl). 2014;127(4):747-52. Chin Med J (Engl). 2014. PMID: 24534234
-
[Short-term efficacy comparison between Ivor-Lewis approach and McKeown approach in minimally invasive esophagectomy].Zhonghua Wei Chang Wai Ke Za Zhi. 2014 Sep;17(9):888-91. Zhonghua Wei Chang Wai Ke Za Zhi. 2014. PMID: 25273657 Chinese.
-
Minimally invasive oesophagectomy versus open esophagectomy for resectable esophageal cancer: a meta-analysis.World J Surg Oncol. 2016 Dec 8;14(1):304. doi: 10.1186/s12957-016-1062-7. World J Surg Oncol. 2016. PMID: 27927246 Free PMC article. Review.
-
Laparoscopic transhiatal esophagectomy for esophageal cancer.Am J Surg. 2005 Jul;190(1):69-74. doi: 10.1016/j.amjsurg.2004.12.004. Am J Surg. 2005. PMID: 15972176 Review.
Cited by
-
Learning Curve for Lymph Node Dissection Around the Recurrent Laryngeal Nerve in McKeown Minimally Invasive Esophagectomy.Front Oncol. 2021 May 20;11:654674. doi: 10.3389/fonc.2021.654674. eCollection 2021. Front Oncol. 2021. PMID: 34094944 Free PMC article.
-
Comparison of short-term outcomes and three yearsurvival between total minimally invasive McKeown and dual-incision esophagectomy.Thorac Cancer. 2017 Mar;8(2):80-87. doi: 10.1111/1759-7714.12404. Epub 2017 Jan 4. Thorac Cancer. 2017. PMID: 28052566 Free PMC article.
-
Reliability and safety of minimally invasive esophagectomy after neoadjuvant chemoradiation: a retrospective study.J Cardiothorac Surg. 2019 May 28;14(1):97. doi: 10.1186/s13019-019-0920-0. J Cardiothorac Surg. 2019. PMID: 31138245 Free PMC article.
-
The value of esophagectomy surgical apgar score (eSAS) in predicting the risk of major morbidity after open esophagectomy.J Thorac Dis. 2016 Jul;8(7):1780-7. doi: 10.21037/jtd.2016.06.28. J Thorac Dis. 2016. PMID: 27499969 Free PMC article.
-
Learning curves in minimally invasive esophagectomy.World J Gastroenterol. 2018 Nov 28;24(44):4974-4978. doi: 10.3748/wjg.v24.i44.4974. World J Gastroenterol. 2018. PMID: 30510372 Free PMC article. Review.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Cuschieri A, Shimi S, Banting S. Endoscopic oesophagectomy through a right thoracoscopic approach. J R Coll Surg Edinb. 1992;37:7–11. - PubMed
-
- Nafteux P, Moons J, Coosemans W, Decaluwé H, Decker G, De Leyn P, Van Raemdonck D, Lerut T. Minimally invasive oesophagectomy: a valuable alternative to open oesophagectomy for the treatment of early oesophageal and gastro-oesophageal junction carcinoma. Eur J Cardiothorac Surg. 2011;40:1455–1463; discussion 1463-1464. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
