

Budd-Chiari syndrome
- PMID: 26668741
- PMCID: PMC4669515
- DOI: 10.1177/2050640615582293
Budd-Chiari syndrome
Abstract
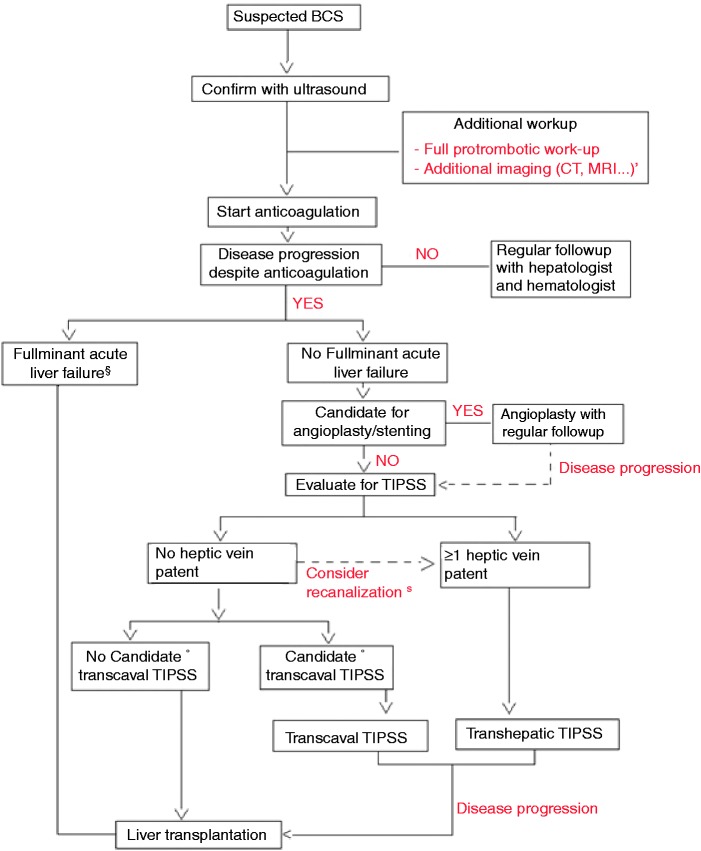
Budd-Chiari syndrome (BCS) is a rare and potentially life-threatening disorder characterized by obstruction of the hepatic outflow tract at any level between the junction of the inferior vena cava with the right atrium and the small hepatic veins. In the West, BCS is a rare hepatic manifestation of one or more underlying prothrombotic risk factors. The most common underlying prothrombotic risk factor is a myeloproliferative disorder, although it is now recognized that almost half of patients have multiple underlying prothrombotic risk factors. Clinical manifestations can be diverse, making BCS a possible differential diagnosis of many acute and chronic liver diseases. The index of suspicion should be very low if there is a known underlying prothrombotic risk factor and new onset of liver disease. Doppler ultrasound is sufficient for confirming the diagnosis, although tomographic imaging (computed tomography (CT) or magnetic resonance imaging (MRI)) is often necessary for further treatment and discussion with a multidisciplinary team. Anticoagulation is the cornerstone of the treatment. Despite the use of anticoagulation, the majority of patients need additional (more invasive) treatment strategies. Algorithms consisting of local angioplasty, TIPS and liver transplantation have been proposed, with treatment choice dictated by a lack of response to a less-invasive treatment regimen. The application of these treatment strategies allows for a five-year survival rate of 90%. In the long term the disease course of BCS can sometimes be complicated by recurrence, progression of the underlying myeloproliferative disorder, or development of post-transplant lymphoma in transplant patients.
Keywords: Budd-Chiari syndrome; TIPS; etiology; liver transplantation; outcome; treatment.
Figures
References
-
- Plessier A, Valla DC. Budd-Chiari syndrome. Semin Liver Dis 2008; 28: 259–269. - PubMed
-
- Darwish MS, Plessier A, Hernandez-Guerra M, et al. Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med 2009; 151: 167–175. - PubMed
-
- Hoekstra J, Janssen HL. Vascular liver disorders (I): Diagnosis, treatment and prognosis of Budd-Chiari syndrome. Neth J Med 2008; 66: 334–339. - PubMed
-
- Qi X, Zhang C, Han G, et al. Prevalence of the JAK2V617F mutation in Chinese patients with Budd-Chiari syndrome and portal vein thrombosis: A prospective study. J Gastroenterol Hepatol 2012; 27: 1036–1043. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
