

Alveolar Dead Space Fraction Discriminates Mortality in Pediatric Acute Respiratory Distress Syndrome
- PMID: 26669646
- PMCID: PMC4740261
- DOI: 10.1097/PCC.0000000000000613
Alveolar Dead Space Fraction Discriminates Mortality in Pediatric Acute Respiratory Distress Syndrome
Abstract
Objectives: Physiologic dead space is associated with mortality in acute respiratory distress syndrome, but its measurement is cumbersome. Alveolar dead space fraction relies on the difference between arterial and end-tidal carbon dioxide (alveolar dead space fraction = (PaCO2 - PetCO2) / PaCO2). We aimed to assess the relationship between alveolar dead space fraction and mortality in a cohort of children meeting criteria for acute respiratory distress syndrome (both the Berlin 2012 and the American-European Consensus Conference 1994 acute lung injury) and pediatric acute respiratory distress syndrome (as defined by the Pediatric Acute Lung Injury Consensus Conference in 2015).
Design: Secondary analysis of a prospective, observational cohort.
Setting: Tertiary care, university affiliated PICU.
Patients: Invasively ventilated children with pediatric acute respiratory distress syndrome.
Interventions: None.
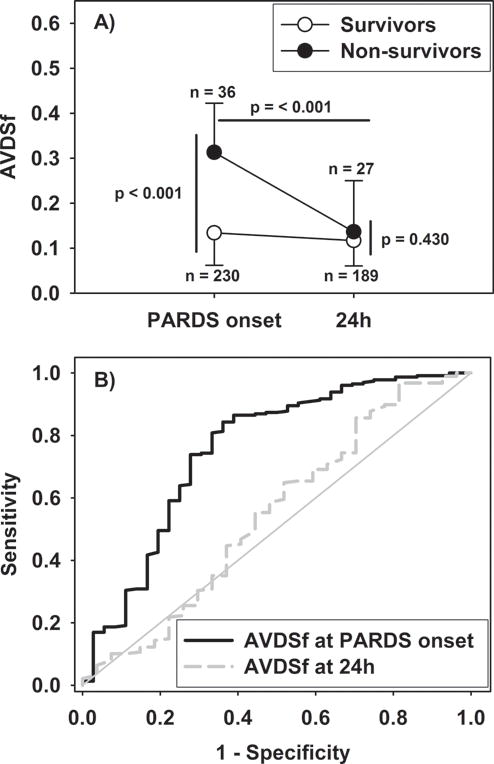
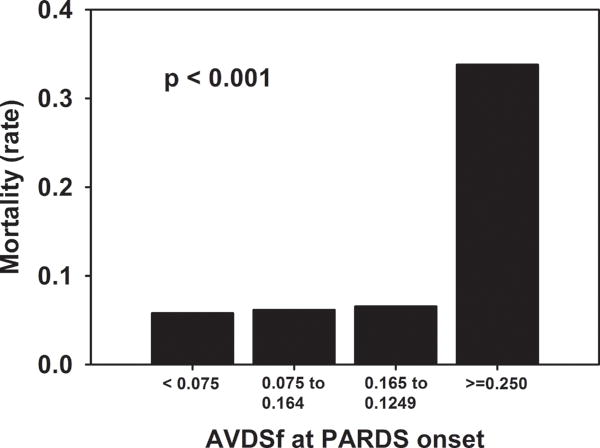
Measurements and main results: Of the 283 children with pediatric acute respiratory distress syndrome, 266 had available PetCO2. Alveolar dead space fraction was lower in survivors (median 0.13; interquartile range, 0.06-0.23) than nonsurvivors (0.31; 0.19-0.42; p < 0.001) at pediatric acute respiratory distress syndrome onset, but not 24 hours after (survivors 0.12 [0.06-0.18], nonsurvivors 0.14 [0.06-0.25], p = 0.430). Alveolar dead space fraction at pediatric acute respiratory distress syndrome onset discriminated mortality with an area under receiver operating characteristic curve of 0.76 (95% CI, 0.66-0.85; p < 0.001), better than either initial oxygenation index or PaO2/FIO2. In multivariate analysis, alveolar dead space fraction at pediatric acute respiratory distress syndrome onset was independently associated with mortality, after adjustment for severity of illness, immunocompromised status, and organ failures.
Conclusions: Alveolar dead space fraction at pediatric acute respiratory distress syndrome onset discriminates mortality and is independently associated with nonsurvival. Alveolar dead space fraction represents a single, useful, readily obtained clinical biomarker reflective of pulmonary and nonpulmonary variables associated with mortality.
Figures
Comment in
-
Pediatric Acute Respiratory Distress Syndrome: Which Child Is Destined to Die?Pediatr Crit Care Med. 2016 Feb;17(2):165-7. doi: 10.1097/PCC.0000000000000632. Pediatr Crit Care Med. 2016. PMID: 26841026 No abstract available.
-
Generalizability Concern of Alveolar Dead Space Fraction of Yehya et al.Pediatr Crit Care Med. 2017 Feb;18(2):204. doi: 10.1097/PCC.0000000000001041. Pediatr Crit Care Med. 2017. PMID: 28157805 No abstract available.
-
The authors reply.Pediatr Crit Care Med. 2017 Feb;18(2):204-205. doi: 10.1097/PCC.0000000000001043. Pediatr Crit Care Med. 2017. PMID: 28157806 No abstract available.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–824. - PubMed
-
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342(18):1301–1308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
