

Asymmetry of parental origin in long QT syndrome: preferential maternal transmission of KCNQ1 variants linked to channel dysfunction
- PMID: 26669661
- PMCID: PMC4970673
- DOI: 10.1038/ejhg.2015.257
Asymmetry of parental origin in long QT syndrome: preferential maternal transmission of KCNQ1 variants linked to channel dysfunction
Abstract
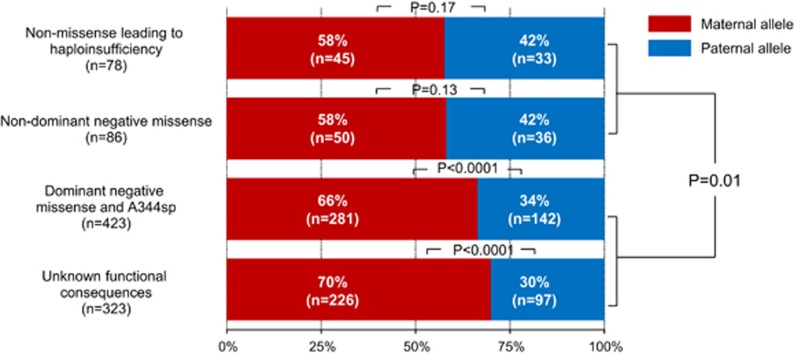
Transmission distortion of disease-causing alleles in long QT syndrome (LQTS) has been reported, suggesting a potential role of KCNQ1 and KCNH2 in reproduction. This study sought to investigate parental transmission in LQTS families according to ethnicity, gene loci (LQT1-3: KCNQ1, KCNH2, and SCN5A) or severity of channel dysfunction. We studied 3782 genotyped members from 679 European and Japanese LQTS families (2748 carriers). We determined grandparental and parental origins of variant alleles in 1903 children and 624 grandchildren, and the grandparental origin of normal alleles in healthy children from 44 three-generation control families. LQTS alleles were more of maternal than paternal origin (61 vs 39%, P<0.001). The ratio of maternally transmitted alleles in LQT1 (66%) was higher than in LQT2 (56%, P<0.001) and LQT3 (57%, P=0.03). Unlike the Mendelian distribution of grandparental alleles seen in control families, variant grandparental LQT1 and LQT2 alleles in grandchildren showed an excess of maternally transmitted grandmother alleles. For LQT1, maternal transmission differs according to the variant level of dysfunction with 68% of maternal transmission for dominant negative or unknown functional consequence variants vs 58% for non-dominant negative and variants leading to haploinsufficiency, P<0.01; however, for LQT2 or LQT3 this association was not significant. An excess of disease-causing alleles of maternal origin, most pronounced in LQT1, was consistently found across ethnic groups. This observation does not seem to be linked to an imbalance in transmission of the LQTS subtype-specific grandparental allele, but to the potential degree of potassium channel dysfunction.
Figures



References
-
- Cerrone M, Priori SG: Genetics of sudden death: focus on inherited channelopathies. Eur Heart J 2011; 32: 2109–2118. - PubMed
-
- Imboden M, Swan H, Denjoy I et al: Female predominance and transmission distortion in the long-QT syndrome. N Engl J Med 2006; 355: 2744–2751. - PubMed
-
- Naumova AK, Greenwood CM, Morgan K: Imprinting and deviation from Mendelian transmission ratios. Genome 2001; 44: 311–320. - PubMed
-
- Naumova AK: Long-QT syndrome. N Engl J Med 2007; 356: 1680, author reply 1680. - PubMed
-
- Kunz L, Roggors C, Mayerhofer A: Ovarian acetylcholine and ovarian KCNQ channels: insights into cellular regulatory systems of steroidogenic granulosa cells. Life Sci 2007; 80: 2195–2198. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
