

ReACT Phase II trial: a critical evaluation of the use of rindopepimut plus bevacizumab to treat EGFRvIII-positive recurrent glioblastoma
- PMID: 26670466
- PMCID: PMC6078156
- DOI: 10.2217/cns.15.38
ReACT Phase II trial: a critical evaluation of the use of rindopepimut plus bevacizumab to treat EGFRvIII-positive recurrent glioblastoma
Retraction in
-
Retraction.CNS Oncol. 2016;5(2):110. doi: 10.2217/cns.16.1. Epub 2016 Jan 6. CNS Oncol. 2016. PMID: 26732311 Free PMC article. No abstract available.
Abstract
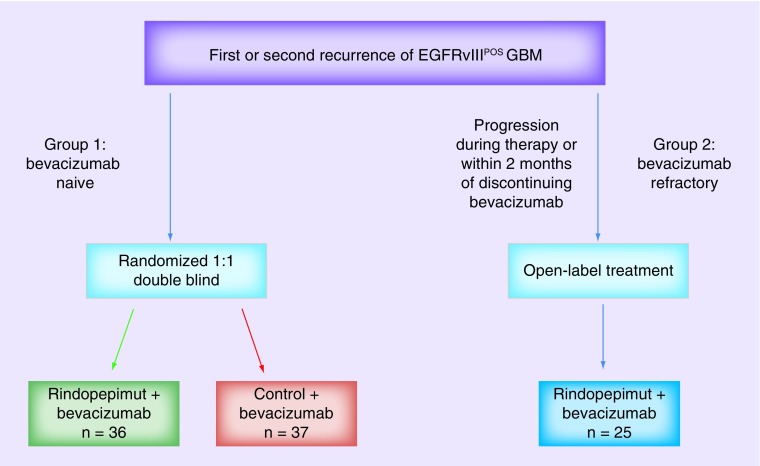
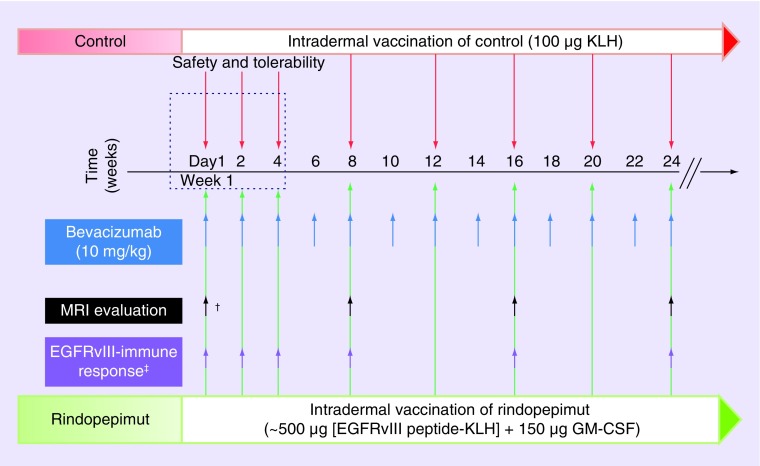
Glioblastoma is the most deadly primary brain tumor in adults and has long represented a therapeutic challenge. Disease recurrence is inevitable, and the management of recurrent disease is complicated by spontaneous or induced tumor heterogeneity which confers resistance to therapy and increased oncogenicity. EGFR and the tumor-specific mutation EGFRvIII is commonly altered in glioblastoma making it an appealing therapeutic target. Immunotherapy is an emerging and promising therapeutic approach to glioma and the EGFRvIII vaccine, rindopepimut, is the first immunotherapeutic drug to enter Phase III clinical trials for glioblastoma. Rindopepimut activates a specific immune response against tumor cells harboring the EGFRvIII protein. This review evaluates the recently completed ReACT Phase II trial using rindopepimut plus bevacizumab in the setting of EGFRvIII-positive recurrent glioblastoma (Clinical Trials identifier: NCT01498328).
Keywords: CDX-110; CNS lymphatics; EGF receptor variant III; EGFRvIII; MGMT; ReACT trial; bevacizumab; immunotherapy; recurrent glioblastoma; rindopepimut; vaccines.
Conflict of interest statement
Figures

References
-
- Stupp R, Mason WP, Van Den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005;352(10):987–996. - PubMed
-
- Weller M, Van Den Bent M, Hopkins K, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014;15(9):e395–e403. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto Phase II clinical trials. J. Clin. Oncol. 1999;17(8):2572–2578. - PubMed
Publication types
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous