

A Comprehensive Study of Extramural Venous Invasion in Colorectal Cancer
- PMID: 26671331
- PMCID: PMC4682925
- DOI: 10.1371/journal.pone.0144987
A Comprehensive Study of Extramural Venous Invasion in Colorectal Cancer
Abstract
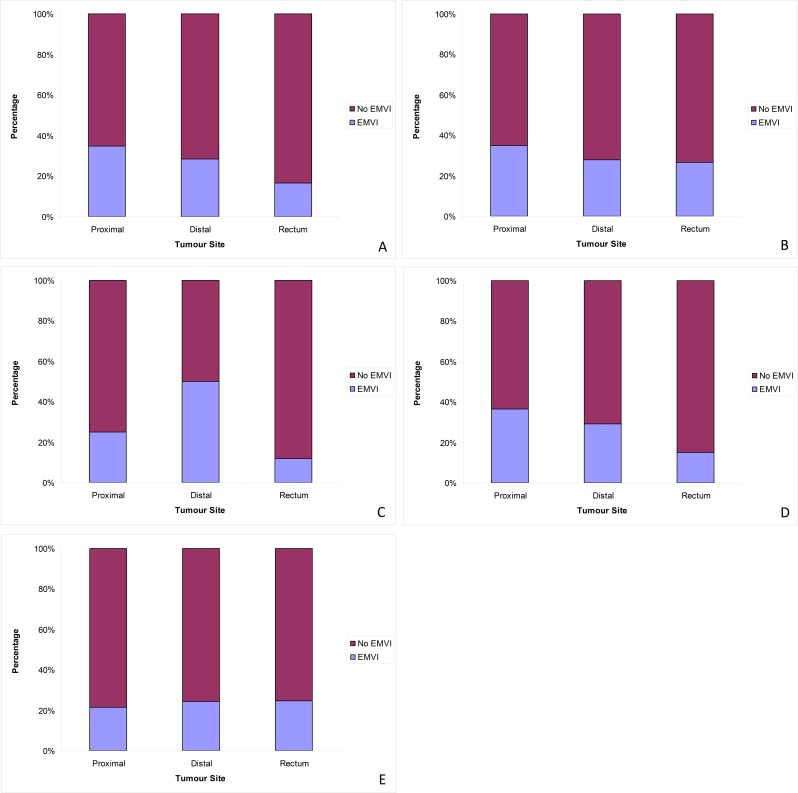
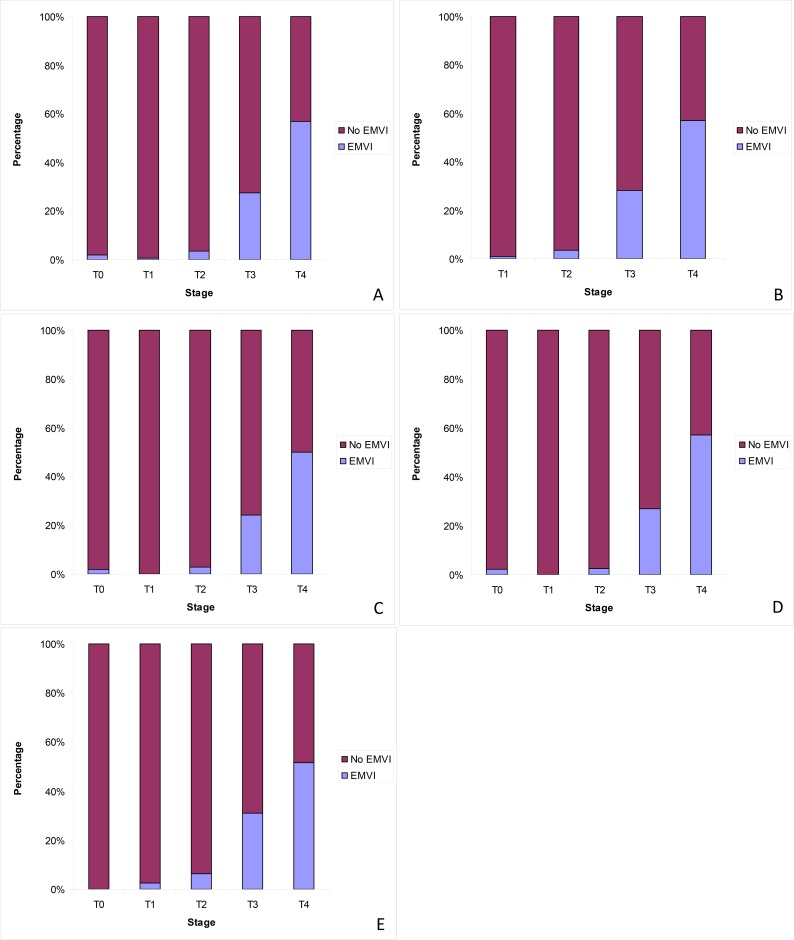
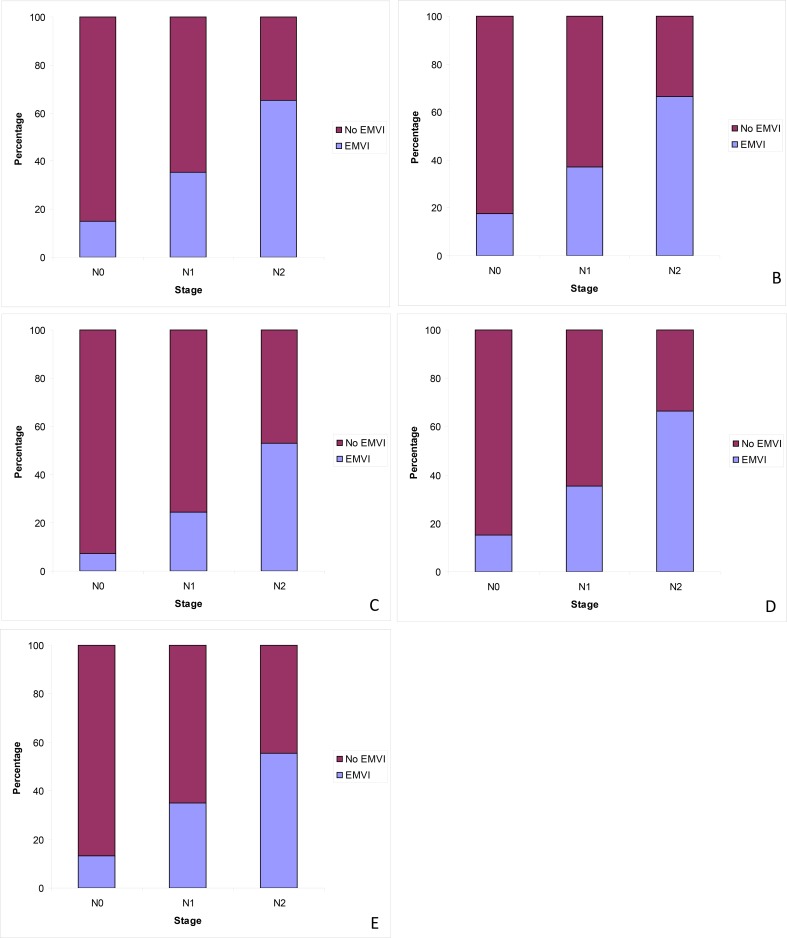
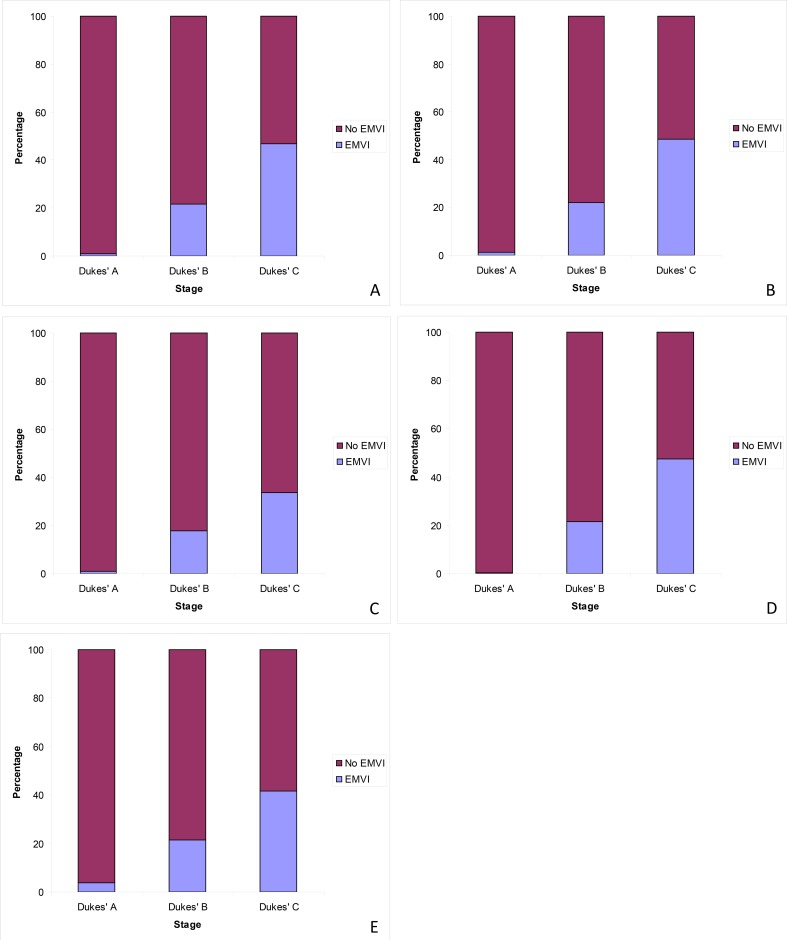
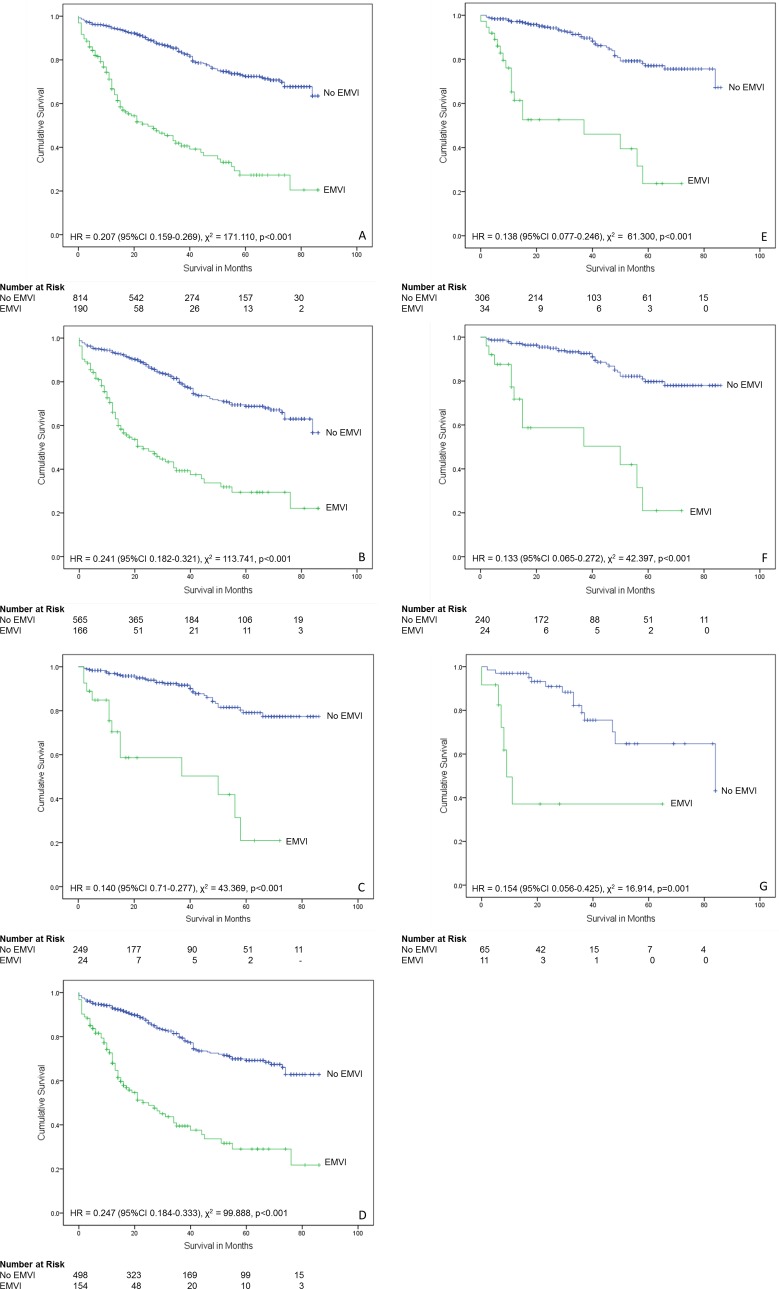
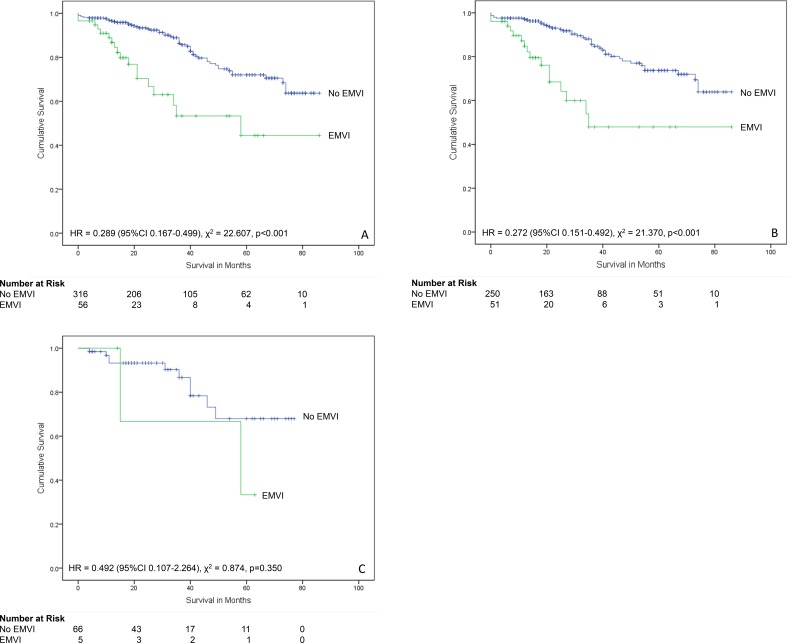
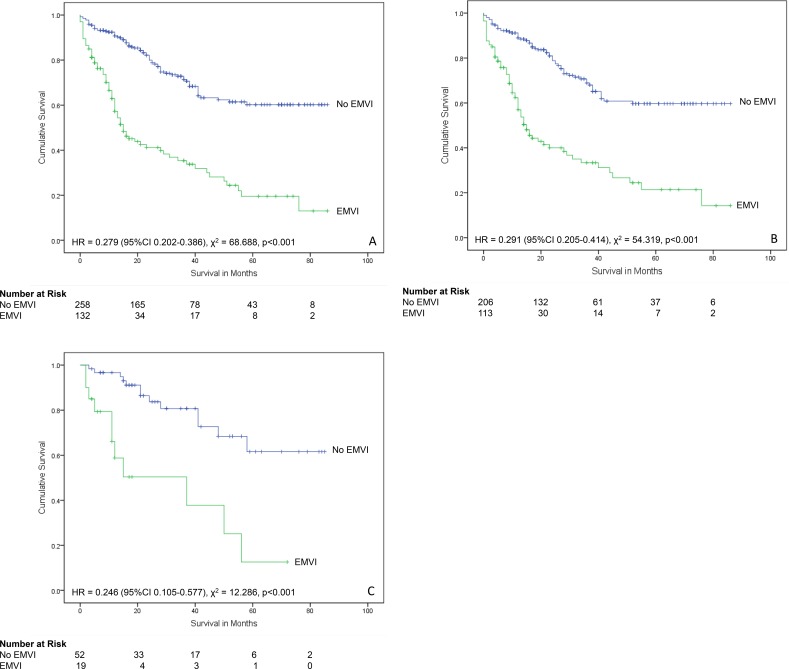
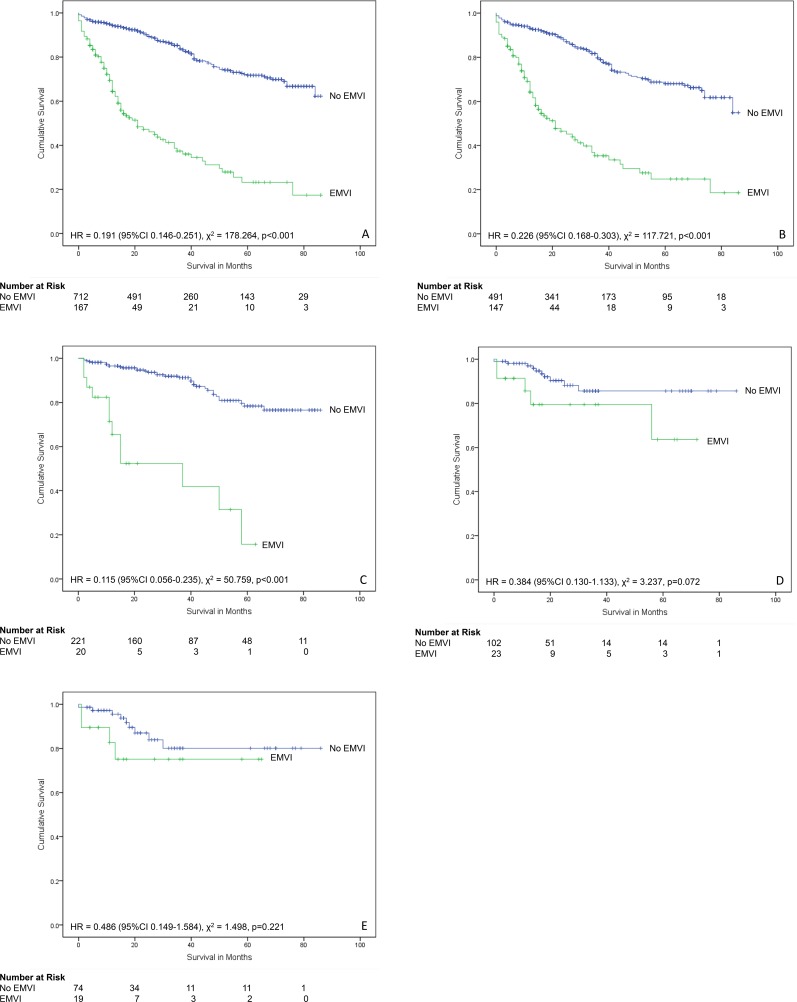
Colorectal cancer is a common malignancy and a leading cause of cancer related death. Cancer staging following resection is key to determining any adjuvant therapy in those patients with high risk disease. In colorectal cancer, tumour stage and lymph node stage are the main pathological factors which have been considered to influence outcome. Increasing emphasis is now being placed on other factors, especially the presence of extramural venous invasion (EMVI). It is important to understand the relationship of EMVI with other pathological factors and to confirm that in an individual centre that EMVI is being detected at an appropriate rate and is of prognostic significance. This comprehensive study assesses the reporting and prognostic significance of EMVI in a single centre, using prospectively collected data from histopathology reports of a cohort of 2405 patients who underwent surgery for colorectal cancer over a nine year period. Overall, EMVI was reported in 27.9% of colorectal cancer excision specimens. In tumours (n = 1928) that had not received neoadjuvant therapy, the presence of EMVI varied significantly depending on tumour site (χ2 = 12.03, p<0.005), tumour stage (χ2 = 268.188, p<0.001), lymph node stage (χ2 = 294.368, p<0.001) and Dukes' stage (χ2 = 253.753, p<0.001). Multivariate analysis confirmed EMVI as a significant independent prognostic indicator (p<0.001). In conclusion, the presence of EMVI as an independent prognostic indicator is shown and is related to other pathological and prognostic factors. This study emphasises the requirement for the accurate identification of EMVI in colorectal cancer excision specimens and also understanding the relationship of EMVI with other prognostic factors.
Conflict of interest statement
Figures
Similar articles
-
Operative and Pathological Factors in Right-Sided Colon Cancers: How Can We Improve the Outcomes?Cureus. 2023 Jan 16;15(1):e33832. doi: 10.7759/cureus.33832. eCollection 2023 Jan. Cureus. 2023. PMID: 36819408 Free PMC article.
-
Incidence of extramural venous invasion in colorectal carcinoma as determined at the invasive tumor front and its prognostic impact.Hum Pathol. 2019 Apr;86:102-107. doi: 10.1016/j.humpath.2018.11.031. Epub 2018 Dec 18. Hum Pathol. 2019. PMID: 30571994
-
The prognostic significance of extramural venous invasion detected by multiple-row detector computed tomography in stage III gastric cancer.Abdom Radiol (NY). 2016 Jul;41(7):1219-26. doi: 10.1007/s00261-015-0627-1. Abdom Radiol (NY). 2016. PMID: 27315092
-
Extramural venous invasion in rectal cancer: overview of imaging, histopathology, and clinical implications.Abdom Radiol (NY). 2019 Jan;44(1):1-10. doi: 10.1007/s00261-018-1673-2. Abdom Radiol (NY). 2019. PMID: 29967984 Review.
-
Systematic review of prognostic importance of extramural venous invasion in rectal cancer.World J Gastroenterol. 2016 Jan 28;22(4):1721-6. doi: 10.3748/wjg.v22.i4.1721. World J Gastroenterol. 2016. PMID: 26819536 Free PMC article.
Cited by
-
Vascular Invasion and Stromal S100A4 Expression at the Invasive Front of Colorectal Cancer are Novel Determinants and Tumor Prognostic Markers.J Cancer. 2017 Jun 2;8(9):1552-1561. doi: 10.7150/jca.18685. eCollection 2017. J Cancer. 2017. PMID: 28775774 Free PMC article.
-
Extramural Venous Invasion as Prognostic Factor of Recurrence in Stage 1 and 2 Colon Cancer.Gastroenterol Res Pract. 2017;2017:1598670. doi: 10.1155/2017/1598670. Epub 2017 Nov 28. Gastroenterol Res Pract. 2017. PMID: 29317863 Free PMC article.
-
MRI Evaluation of Extramural Venous Invasion (EMVI) with Rectal Carcinoma Using High Resolution T2 and Combination of High Resolution T2 and Contrast Enhanced T1 Weighted Imaging.Acta Inform Med. 2021 Jun;29(2):113-117. doi: 10.5455/aim.2021.29.113-117. Acta Inform Med. 2021. PMID: 34584334 Free PMC article.
-
Risk Factors for Distant Metastasis in T3 T4 Rectal Cancer.Clin Med Insights Oncol. 2024 Feb 5;18:11795549241227423. doi: 10.1177/11795549241227423. eCollection 2024. Clin Med Insights Oncol. 2024. PMID: 38322665 Free PMC article.
-
The value of tumor deposits in evaluating colorectal cancer survival and metastasis: a population-based retrospective cohort study.World J Surg Oncol. 2022 Feb 21;20(1):41. doi: 10.1186/s12957-022-02501-9. World J Surg Oncol. 2022. PMID: 35189906 Free PMC article.
References
-
- Loughrey M, Quirke P, Shepherd NA. Standards and datasets for reporting cancers Dataset for colorectal cancer histopathology reports. 3rd edition The Royal College of Pathologists, London, UK, 2014. Available: http://www.rcpath.org/publications-media/publications/datasets/colorecta...
-
- Gibson KM, Chan C, Chapuis PH, Dent OF, Bokey L. Mural and extramural venous invasion and prognosis in colorectal Cancer. Dis Colon Rectum 2014;57:919–926 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
