

Diagnosis and treatment of pancreatic pseudocysts and cystic tumors based on own material and quoted literature
- PMID: 26673675
- PMCID: PMC4603218
- DOI: 10.15557/JoU.2013.0028
Diagnosis and treatment of pancreatic pseudocysts and cystic tumors based on own material and quoted literature
Abstract
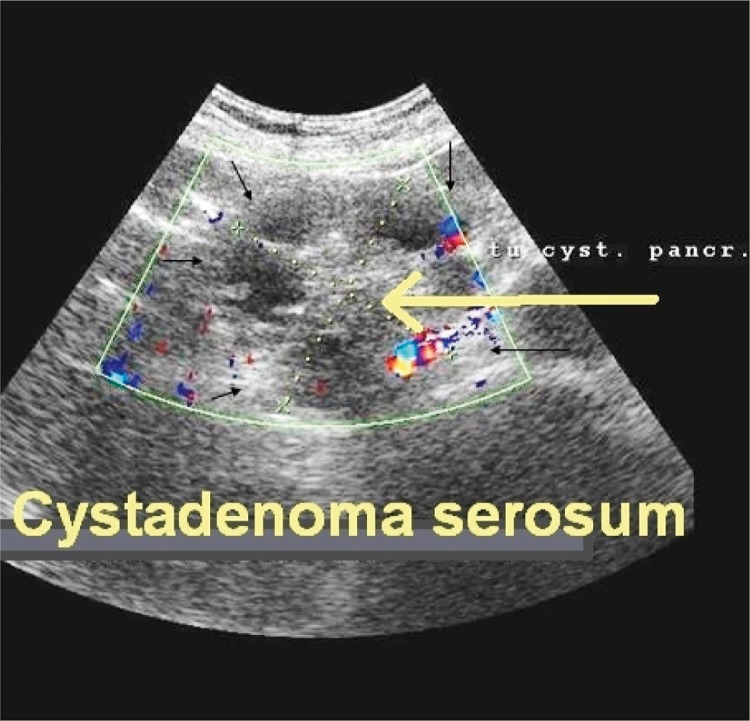
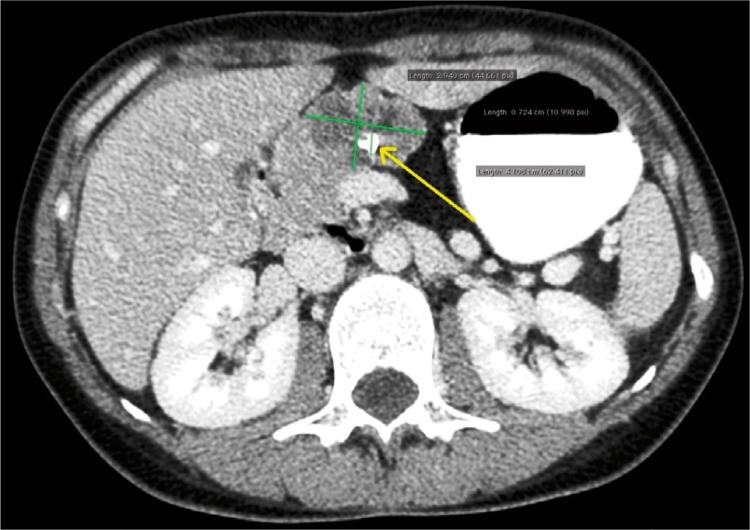
Pseudocysts constitute the most basic cystic lesions of the pancreas. Symptomatic cysts may be treated by means of both minimally invasive methods and surgery. Currently, it is believed that approximately 5% of cystic lesions in the pancreas may in fact, be neoplastic cystic tumors. Their presence is manifested by generally irregular multilocular structures, solid nodules inside the cyst or in the pancreatic duct, frequently vascularized, as well as fragmentary thickening of the cystic wall or septation.
Aim: The aim of this paper was to present current management, both diagnostic and therapeutic, in patients with pancreatic pseudocysts and cystic tumors. The article has been written based on the material collected and prepared in the author's Department as well as on the basis of current reports found in the quoted literature.
Material and methods results: In 2000-2012, the Second Department of General, Gastrointestinal and Oncological Surgery of the Alimentary Tract treated 179 patients with cystic lesions in the region of the pancreas. This group comprised 12 cases of cystic tumors and 167 pseudocysts. Twenty-three patients (13.8%) were monitored only and 144 received procedural treatment. Out of the latter group, 75 patients underwent drainage procedures and 48 were qualified to endoscopic cystogastrostomy or cystoduodenostomy. The endoscopic procedure was unsuccessful in 11 cases (23%). In a group of patients with a pancreatic cystic tumor (12 patients), 6 of them (50%) underwent therapeutic resection of the tumor with adequate fragment of the gland.
Conclusions: Endoscopic drainage is an effective and safe method of minimally invasive treatment of pancreatic cysts. The patients who do not qualify to endoscopic procedures require surgical treatment. The differentiation of a neoplasm from a typical cyst is of fundamental significance for the selection of the treatment method.
Do podstawowych zmian o typie torbieli trzustki należą torbiele rzekome. Objawowe torbiele można leczyć zarówno z wykorzystaniem technik małoinwazyjnych, jak i chirurgicznie. Obecnie przyjmuje się, że w około 5% torbielowatych zmian w trzustce możemy mieć do czynienia z nowotworowymi guzami torbielowatymi. Za ich obecnością przemawiają struktury wielokomorowe, najczęściej nieregularne, lite guzki we wnętrzu torbieli lub w przewodzie trzustkowym, często unaczynione, oraz odcinkowe pogrubienie ściany torbieli lub przegrody.
Cel pracy: Celem niniejszej pracy jest przedstawienie obecnej taktyki postępowania zarówno diagnostycznego, jak i terapeutycznego u chorych z pseudotorbielami oraz torbielowatymi guzami trzustki. Praca została napisana na podstawie materiału zebranego i przygotowanego w Klinice autora oraz współczesnych doniesień z zaprezentowanego piśmiennictwa.
Materiał i metoda wyniki: W latach 2000–2012 w II Klinice Chirurgii Ogólnej, Gastroenterologicznej i Nowotworów Układu Pokarmowego przebywało 179 chorych z torbielowatymi zmianami w obrębie trzustki, w tej grupie stwierdzono 12 przypadków guzów torbielowatych oraz 167 zmian o charakterze rzekomych torbieli – u 23 pacjentów (13,8%) prowadzono jedynie obserwację, pozostałych 144 leczono zabiegowo. U 75 wykonano zabieg drenażowy na drodze operacyjnej, 48 chorych zakwalifikowano do endoskopowej cystogastrostomii lub cystoduodenostomii. Zabieg endoskopowy nie powiódł się u 11 leczonych (23%). W grupie pacjentów z guzem torbielowatym trzustki na 12 badanych u 6 (50%) wykonano leczniczą resekcję guza z odpowiednią częścią narządu.
Wnioski: Zabiegi endoskopowego drenażu torbieli trzustki stanowią efektywną i bezpieczną metodę małoinwazyjnego leczenia. Chorzy niezakwalifikowani do zabiegu endoskopowego wymagają leczenia operacyjnego. Odróżnienie nowotworu od typowej torbieli trzustki ma podstawowe znaczenie dla kwalifikacji do sposobu leczenia.
Keywords: imaging diagnosis; pancreatic cystic tumors; pancreatic cysts; principles of qualification to treatment; treatment method.
Figures

















References
-
- Lipiński M, Degowska M, Rydzewska G. Zmiany torbielowate w trzustce. Przegląd Gastroenterologiczny. 2007;2:315–319.
-
- Kim YH, Saini S, Sahani D, Hahn PF, Mueller PR, Auh YH. Imaging diagnosis of cystic pancreatic lesions: pseudocyst versus nonpseudocyst. Radiographics. 2005;25:671–685. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources