

Endoscopy vs surgery in the treatment of early gastric cancer: Systematic review
- PMID: 26675093
- PMCID: PMC4674737
- DOI: 10.3748/wjg.v21.i46.13177
Endoscopy vs surgery in the treatment of early gastric cancer: Systematic review
Abstract
Aim: To report a systematic review, establishing the available data to an unpublished 2a strength of evidence, better handling clinical practice.
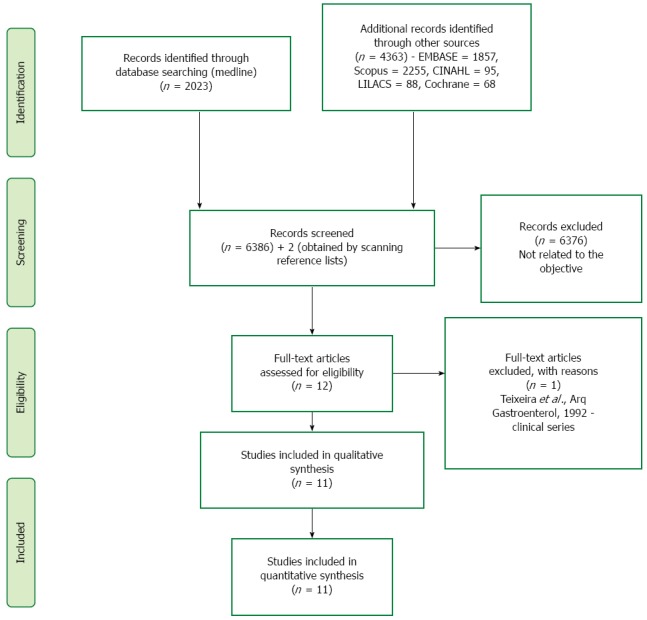
Methods: A systematic review was performed using MEDLINE, EMBASE, Cochrane, LILACS, Scopus and CINAHL databases. Information of the selected studies was extracted on characteristics of trial participants, inclusion and exclusion criteria, interventions (mainly, mucosal resection and submucosal dissection vs surgical approach) and outcomes (adverse events, different survival rates, mortality, recurrence and complete resection rates). To ascertain the validity of eligible studies, the risk of bias was measured using the Newcastle-Ottawa Quality Assessment Scale. The analysis of the absolute risk of the outcomes was performed using the software RevMan, by computing risk differences (RD) of dichotomous variables. Data on RD and 95%CIs for each outcome were calculated using the Mantel-Haenszel test and inconsistency was qualified and reported in χ(2) and the Higgins method (I (2)). Sensitivity analysis was performed when heterogeneity was higher than 50%, a subsequent assay was done and other findings were compiled.
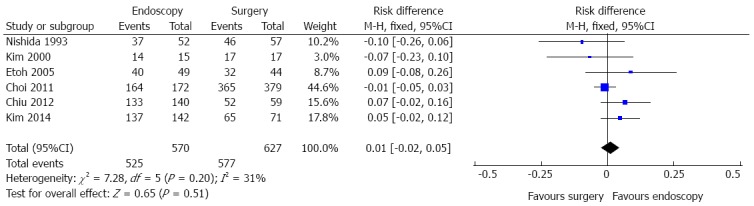
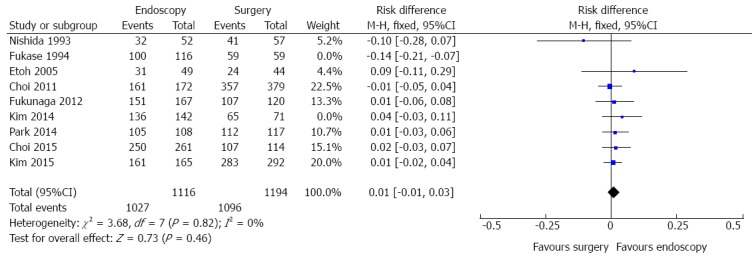
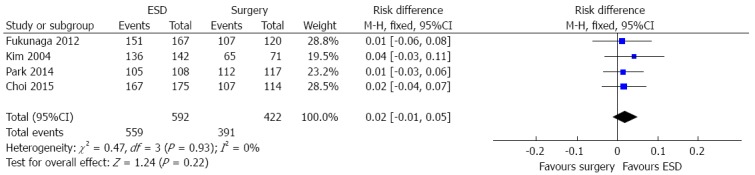
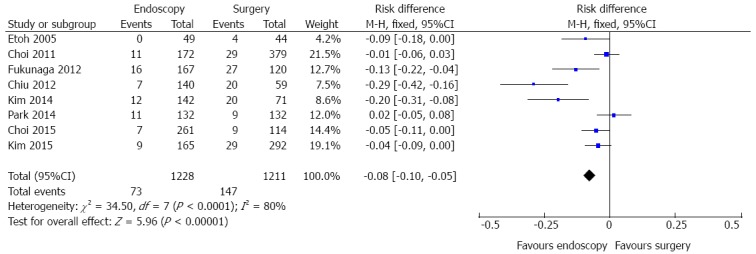
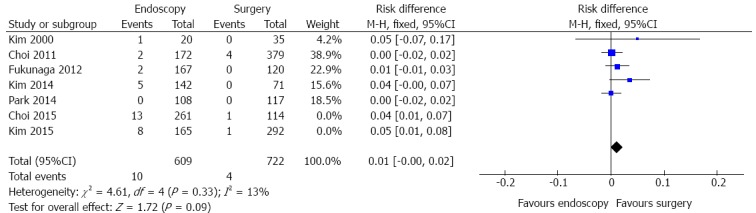
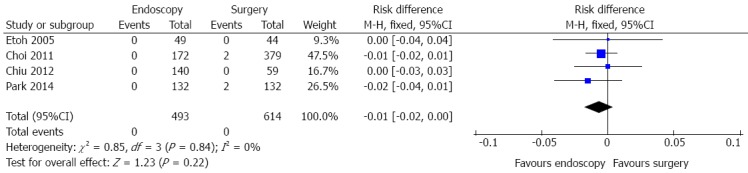
Results: Eleven retrospective cohort studies were selected. The included records involved 2654 patients with early gastric cancer that filled the absolute or expanded indications for endoscopic resection. Three-year survival data were available for six studies (n = 1197). There were no risk differences (RD) after endoscopic and surgical treatment (RD = 0.01, 95%CI: -0.02-0.05, P = 0.51). Five-year survival data (n = 2310) showed no difference between the two groups (RD = 0.01, 95%CI: -0.01-0.03, P = 0.46). Recurrence data were analized in five studies (1331 patients) and there was no difference between the approaches (RD = 0.01, 95%CI: -0.00-0.02, P = 0.09). Adverse event data were identified in eight studies (n = 2439). A significant difference was detected (RD = -0.08, 95%CI: -0.10--0.05, P < 0.05), demonstrating better results with endoscopy. Mortality data were obtained in four studies (n = 1107). There was no difference between the groups (RD = -0.01, 95%CI: -0.02-0.00, P = 0.22).
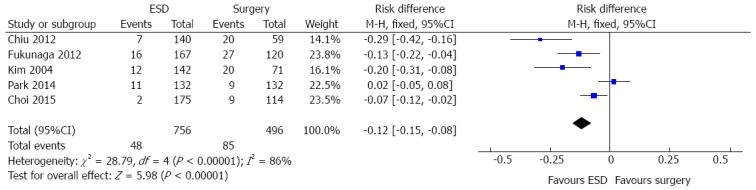
Conclusion: Three-, 5-year survival, recurrence and mortality are similar for both groups. Considering complication, endoscopy is better and, analyzing complete resection data, it is worse than surgery.
Keywords: Endoscopy; Gastrectomy; Gastric cancer; Gastroscopy; Surgery; Systematic review.
Figures
Similar articles
-
Endoscopic stenting for inoperable malignant biliary obstruction: A systematic review and meta-analysis.World J Gastroenterol. 2015 Dec 21;21(47):13374-85. doi: 10.3748/wjg.v21.i47.13374. World J Gastroenterol. 2015. PMID: 26715823 Free PMC article.
-
Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding.Cochrane Database Syst Rev. 2013 Nov 15;2013(11):CD010241. doi: 10.1002/14651858.CD010241.pub2. Cochrane Database Syst Rev. 2013. PMID: 24234875 Free PMC article.
-
Laparoscopic versus open gastrectomy for gastric cancer.Cochrane Database Syst Rev. 2016 Mar 31;3(3):CD011389. doi: 10.1002/14651858.CD011389.pub2. Cochrane Database Syst Rev. 2016. PMID: 27030300 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
Cited by
-
Prognostic factors for ESD of early gastric cancers: a systematic review and meta-analysis.Endosc Int Open. 2020 Sep;8(9):E1144-E1155. doi: 10.1055/a-1201-3089. Epub 2020 Aug 31. Endosc Int Open. 2020. PMID: 32904802 Free PMC article. Review.
-
Beyond the Guidelines: The Grey Zones of the Management of Gastric Cancer. Consensus Statements from the Gastric Cancer Italian Network (GAIN).Cancers (Basel). 2021 Mar 15;13(6):1304. doi: 10.3390/cancers13061304. Cancers (Basel). 2021. PMID: 33804024 Free PMC article. Review.
-
The Pilot Study on Detecting Perforation with Abdominal Ultrasound During Gastric Endoscopic Submucosal Dissection.Diagnostics (Basel). 2025 Jan 31;15(3):335. doi: 10.3390/diagnostics15030335. Diagnostics (Basel). 2025. PMID: 39941265 Free PMC article.
-
Effect and cost-effectiveness of national gastric cancer screening in Japan: a microsimulation modeling study.BMC Med. 2020 Sep 14;18(1):257. doi: 10.1186/s12916-020-01729-0. BMC Med. 2020. PMID: 32921305 Free PMC article.
-
Endoscopic Submucosal Dissection versus Surgery for Undifferentiated-Type Early Gastric Cancer: A Systematic Review and Meta-Analysis.Clin Endosc. 2021 Mar;54(2):202-210. doi: 10.5946/ce.2020.121. Epub 2021 Feb 17. Clin Endosc. 2021. PMID: 33596638 Free PMC article.
References
-
- 2012. International Association of Cancer Registry (IACR): GLOBOCAN.
-
- Murakami T. Early cancer of the stomach. World J Surg. 1979;3:685–692. - PubMed
-
- Folli S, Morgagni P, Roviello F, De Manzoni G, Marrelli D, Saragoni L, Di Leo A, Gaudio M, Nanni O, Carli A, et al. Risk factors for lymph node metastases and their prognostic significance in early gastric cancer (EGC) for the Italian Research Group for Gastric Cancer (IRGGC) Jpn J Clin Oncol. 2001;31:495–499. - PubMed
-
- Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc. 2003;57:567–579. - PubMed
-
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3) Gastric Cancer. 2011;14:113–123. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
