

Hypercalcemia of malignancy and new treatment options
- PMID: 26675713
- PMCID: PMC4675637
- DOI: 10.2147/TCRM.S83681
Hypercalcemia of malignancy and new treatment options
Abstract
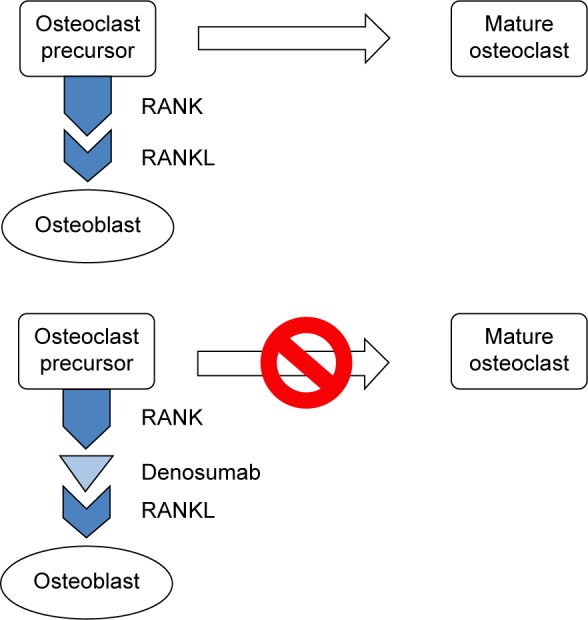
Hypercalcemia of malignancy affects up to one in five cancer patients during the course of their disease. It is associated with both liquid malignancies, commonly multiple myeloma, leukemia, and non-Hodgkins lymphoma and solid cancers, particularly breast and renal carcinomas as well as squamous cell carcinomas of any organ. The clinical manifestations of hypercalcemia are generally constitutional in nature and not specific to the inciting malignancy. Such physical manifestations can range from malaise to lethargy and confusion. Constipation and anorexia are common. Acute kidney injury is likely the most frequently encountered manifestation of end organ damage. Symptomatology is closely linked to both the absolute elevation of serum calcium levels and the rapidity of calcium rise. The majority of cases are humoral in etiology and related to parathyroid hormone-related protein (PTHrP). Approximately 20% of cases are the result of direct bone metastasis with extra-renal 1,25-dihydroxyvitamin D (calcitriol) and ectopic parathyroid hormone production likely accounting for less than 1% of cases. The diagnosis of hypercalcemia of malignancy is confirmed either by an elevated PTHrP or by an evidence of bone metastasis in the appropriate clinical setting. Treatment is predicated on the patient's symptoms and absolute serum calcium level. Interventions are aimed at lowering the serum calcium concentration by inhibiting bone resorption and increasing urinary calcium excretion, the former accomplished via bisphosphonate therapy and the latter with aggressive hydration. Novel therapies for refractory disease include denosumab, a monoclonal antibody against the receptor activator of nuclear factor κB ligand, and the calcimimetic cinacalcet. Finally, anti-PTHrP antibodies have been successfully deployed in animal models of disease. Despite the efficacy of the above therapies, hypercalcemia of malignancy portends an ominous prognosis, indicating advanced and often refractory cancer with survival on the order of months.
Keywords: bisphosphonates; calcitonin; cinacalcet; denosumab; hypercalcemia of malignancy parathyroid hormone; parathyroid hormone-related protein.
Figures
References
-
- Horwitz M, Hodak S, Stewart A. Non-parathyroid hypercalcemia. In: Favus M, editor. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. Washington, DC; American Society of Bone and Mineral Research; 2008. pp. 307–312.
-
- Stewart AF. Clinical practice. Hypercalcemia associated with cancer. New Engl J Med. 2005;352(4):373–379. - PubMed
-
- Rosner MH, Dalkin AC. Onco-nephrology: the pathophysiology and treatment of malignancy-associated hypercalcemia. Clin J Am Soc Nephrol. 2012;7(10):1722–1729. - PubMed
-
- Burt ME, Brennan MF. Incidence of hypercalcemia and malignant neoplasm. Arch Surg. 1980;115(6):704–707. - PubMed
-
- Vassilopoulou-Sellin R, Newman BM, Taylor SH, Guinee VF. Incidence of hypercalcemia in patients with malignancy referred to a comprehensive cancer center. Cancer. 1993;71(4):1309–1312. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
