

Detection of Airway Colonization by Aspergillus fumigatus by Use of Electronic Nose Technology in Patients with Cystic Fibrosis
- PMID: 26677251
- PMCID: PMC4767968
- DOI: 10.1128/JCM.02214-15
Detection of Airway Colonization by Aspergillus fumigatus by Use of Electronic Nose Technology in Patients with Cystic Fibrosis
Erratum in
-
Correction for de Heer et al., Detection of Airway Colonization by Aspergillus fumigatus by Use of Electronic Nose Technology in Patients with Cystic Fibrosis.J Clin Microbiol. 2016 Jul;54(7):1926. doi: 10.1128/JCM.00748-16. J Clin Microbiol. 2016. PMID: 27343292 Free PMC article. No abstract available.
Abstract
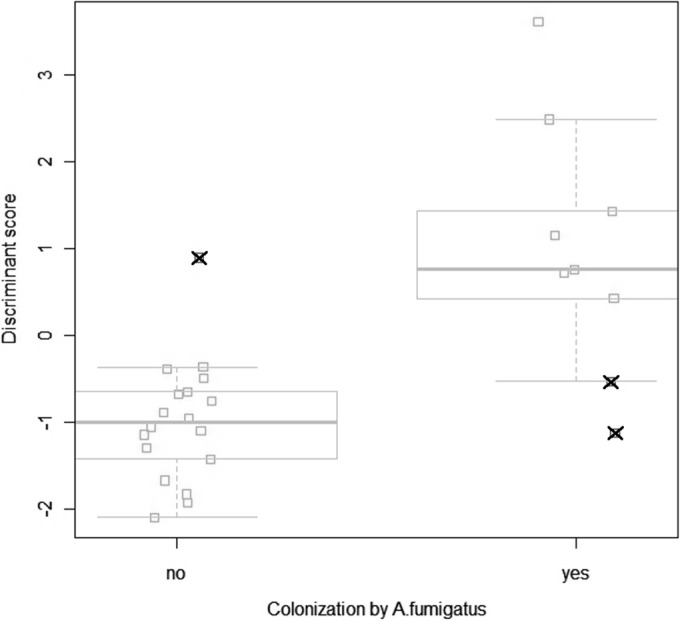
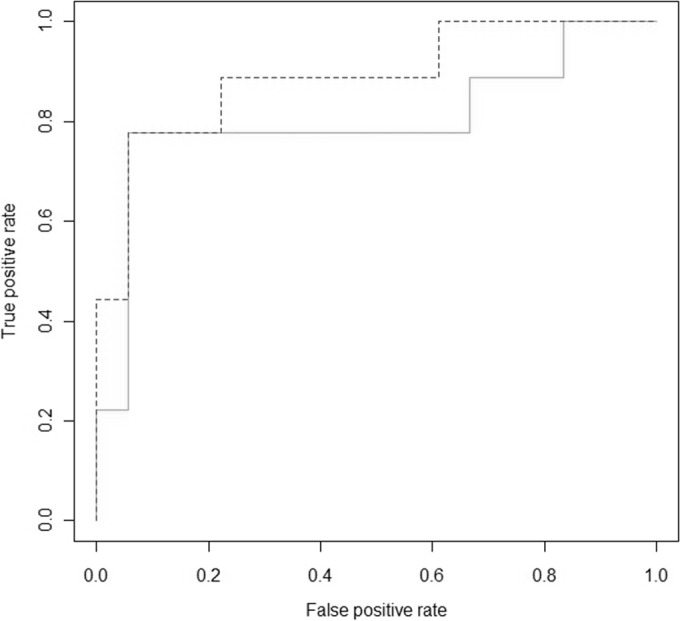
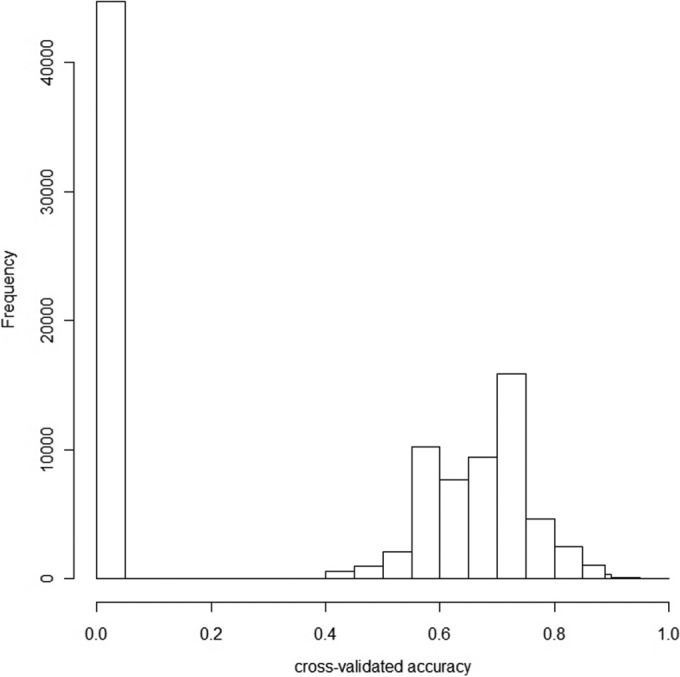
Currently, there is no noninvasive test that can reliably diagnose early invasive pulmonary aspergillosis (IA). An electronic nose (eNose) can discriminate various lung diseases through an analysis of exhaled volatile organic compounds. We recently published a proof-of-principle study showing that patients with prolonged chemotherapy-induced neutropenia and IA have a distinct exhaled breath profile (or breathprint) that can be discriminated with an eNose. An eNose is cheap and noninvasive, and it yields results within minutes. We determined whether Aspergillus fumigatus colonization may also be detected with an eNose in cystic fibrosis (CF) patients. Exhaled breath samples of 27 CF patients were analyzed with a Cyranose 320. Culture of sputum samples defined the A. fumigatus colonization status. eNose data were classified using canonical discriminant analysis after principal component reduction. Our primary outcome was cross-validated accuracy, defined as the percentage of correctly classified subjects using the leave-one-out method. The P value was calculated by the generation of 100,000 random alternative classifications. Nine of the 27 subjects were colonized by A. fumigatus. In total, 3 subjects were misclassified, resulting in a cross-validated accuracy of the Cyranose detecting IA of 89% (P = 0.004; sensitivity, 78%; specificity, 94%). Receiver operating characteristic (ROC) curve analysis showed an area under the curve (AUC) of 0.89. The results indicate that A. fumigatus colonization leads to a distinctive breathprint in CF patients. The present proof-of-concept data merit external validation and monitoring studies.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Electronic nose technology for detection of invasive pulmonary aspergillosis in prolonged chemotherapy-induced neutropenia: a proof-of-principle study.J Clin Microbiol. 2013 May;51(5):1490-5. doi: 10.1128/JCM.02838-12. Epub 2013 Mar 6. J Clin Microbiol. 2013. PMID: 23467602 Free PMC article.
-
eNose technology can detect and classify human pathogenic molds in vitro: a proof-of-concept study of Aspergillus fumigatus and Rhizopus oryzae.J Breath Res. 2016 Jul 22;10(3):036008. doi: 10.1088/1752-7155/10/3/036008. J Breath Res. 2016. PMID: 27447026
-
Exhaled breath analysis using electronic nose in cystic fibrosis and primary ciliary dyskinesia patients with chronic pulmonary infections.PLoS One. 2014 Dec 26;9(12):e115584. doi: 10.1371/journal.pone.0115584. eCollection 2014. PLoS One. 2014. PMID: 25542036 Free PMC article.
-
Novel diagnostics: progress toward a breath test for invasive Aspergillus fumigatus.Med Mycol. 2011 Apr;49 Suppl 1:S54-61. doi: 10.3109/13693786.2010.508187. Epub 2010 Aug 26. Med Mycol. 2011. PMID: 20795766 Review.
-
The co-colonization prevalence of Pseudomonas aeruginosa and Aspergillus fumigatus in cystic fibrosis: A systematic review and meta-analysis.Microb Pathog. 2018 Dec;125:122-128. doi: 10.1016/j.micpath.2018.09.010. Epub 2018 Sep 11. Microb Pathog. 2018. PMID: 30217514
Cited by
-
Aspergillus Is Inhibited by Pseudomonas aeruginosa Volatiles.J Fungi (Basel). 2020 Jul 25;6(3):118. doi: 10.3390/jof6030118. J Fungi (Basel). 2020. PMID: 32722412 Free PMC article.
-
Rational lung tissue and animal models for rapid breath tests to determine pneumonia and pathogens.Am J Transl Res. 2017 Nov 15;9(11):5116-5126. eCollection 2017. Am J Transl Res. 2017. PMID: 29218109 Free PMC article.
-
Potential of the Electronic Nose for the Detection of Respiratory Diseases with and without Infection.Int J Mol Sci. 2020 Dec 10;21(24):9416. doi: 10.3390/ijms21249416. Int J Mol Sci. 2020. PMID: 33321951 Free PMC article. Review.
-
Novel cutting-edge metabolite-based diagnostic tools for aspergillosis.PLoS Pathog. 2017 Sep 7;13(9):e1006486. doi: 10.1371/journal.ppat.1006486. eCollection 2017 Sep. PLoS Pathog. 2017. PMID: 28880911 Free PMC article. Review. No abstract available.
-
CFTR Modulator Therapies in Pediatric Cystic Fibrosis: Focus on Ivacaftor.Expert Opin Orphan Drugs. 2016 Oct;4(10):1033-1042. doi: 10.1080/21678707.2016.1226800. Epub 2016 Sep 13. Expert Opin Orphan Drugs. 2016. PMID: 28042521 Free PMC article.
References
-
- Dettenkofer M, Wenzler-Röttele S, Babikir R, Bertz H, Ebner W, Meyer E, Rüden H, Gastmeier P, Daschner FD, Hospital Infection Surveillance System for Patients with Hematologic/Oncologic Malignancies Study Group . 2005. Surveillance of nosocomial sepsis and pneumonia in patients with a bone marrow or peripheral blood stem cell transplant: a multicenter project. Clin Infect Dis 40:926–931. doi:10.1086/428046. - DOI - PubMed
-
- Cornillet A, Camus C, Nimubona S, Gandemer V, Tattevin P, Belleguic C, Chevrier S, Meunier C, Lebert C, Aupe M, Caulet-Maugendre S, Faucheux M, Lelong B, Leray E, Guiguen C, Gangneux JP. 2006. Comparison of epidemiological, clinical, and biological features of invasive aspergillosis in neutropenic and nonneutropenic patients: a 6-year survey. Clin Infect Dis 43:577–584. doi:10.1086/505870. - DOI - PubMed
-
- Robenshtok E, Gafter-Gvili A, Goldberg E, Weinberger M, Yeshurun M, Leibovici L, Paul M. 2007. Antifungal prophylaxis in cancer patients after chemotherapy or hematopoietic stem-cell transplantation: systematic review and meta-analysis. J Clin Oncol 25:5471–5489. doi:10.1200/JCO.2007.12.3851. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
