

The incidence of un-indicated preoperative testing in a tertiary academic ambulatory center: a retrospective cohort study
- PMID: 26677410
- PMCID: PMC4681056
- DOI: 10.1186/s13741-015-0023-y
The incidence of un-indicated preoperative testing in a tertiary academic ambulatory center: a retrospective cohort study
Abstract
Background: Despite existing evidence and guidelines advocating for appropriate risk stratification, ambulatory surgery in low-risk patients continues to be accompanied by a battery of routine tests prior to surgery. Using a single-center retrospective cohort study, we aimed to quantify the incidence of un-indicated preoperative testing in an academic ambulatory center by utilizing recommendations by the recently developed American Society of Anesthesiology (ASA) "Choosing Wisely" Top-5 list.
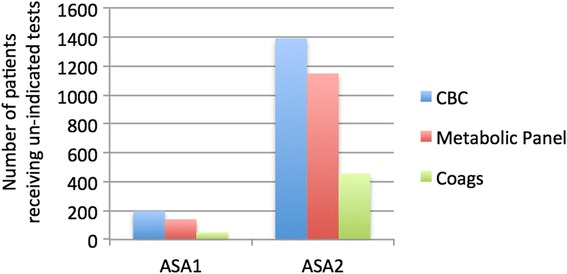
Methods: We utilized data from the EPIC medical records of 3111 patients who had ambulatory surgery at the Hospital of the University of Pennsylvania during a 6-month period. Data were abstracted from laboratory studies- complete blood count, electrolyte panel, coagulation studies, and cardiac studies-stress test, and echocardiogram obtained within 30 days prior to surgery. Preoperative tests obtained from each patient were categorized into "indicated" (ASA ≥ 3) and "un-indicated" (ASA 1 and 2) tests, and percentages were reported.
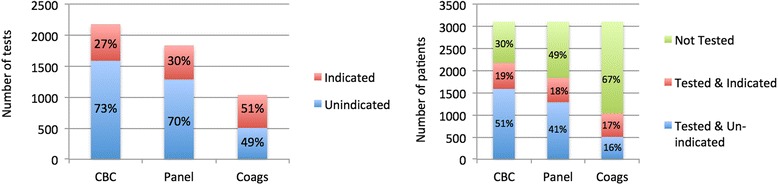
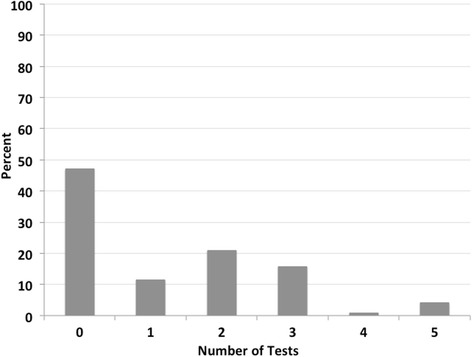
Results: During the study period, 52.9 % (95 % confidence interval (CI) 37.6-66.4) of all patients had at least one un-indicated laboratory test performed preoperatively. Further analysis revealed variation in the incidence of preoperative ordering between tests; 73 % of all complete blood counts (CBCs), 70 % of all metabolic panels, and 49 % of all coagulation studies were considered un-indicated by "Top-5 List" criteria. Stated differently, of the patients included in the sample, 51 % of patients received an un-indicated CBC, 41 % an un-indicated metabolic panel, and 16 % un-indicated coagulation studies. Twelve percent of "any un-indicated preoperative test" were obtained from ASA 1 healthy patients. Of the 587 patients less than 36 years old, 331 (56 %) had at least one test that was deemed un-indicated. Forty-one patients had either an echocardiogram or stress test ordered and performed within 30 days of surgery. Of these, eight (19.5 %) studies were un-indicated as determined by chart review.
Conclusions: The incidence of ordering "at least one un-indicated preoperative test" in low-risk patients undergoing low-risk surgery remains high even in academic tertiary institutions. In the emerging era of optimizing patient safety and financial accountability, further studies are needed to better understand the problem of overuse while identifying modifiable attitudes and institutional influences on perioperative practices among all stakeholders involved. Such information would drive the development of feasible interventions.
Keywords: ASA (American Society of Anesthesiology); Ambulatory; Laboratory test (complete blood count, metabolic panel, coagulation studies); Low risk; Preoperative testing; Routine; Un-indicated.
Figures
Similar articles
-
Utility of Routine Preoperative Laboratory Testing for Low-risk Patients in Ambulatory Gynecologic Surgery.J Minim Invasive Gynecol. 2021 May;28(5):1033-1040.e1. doi: 10.1016/j.jmig.2021.01.001. Epub 2021 Jan 8. J Minim Invasive Gynecol. 2021. PMID: 33429058
-
Current preoperative testing practices in ambulatory surgery are widely disparate: a survey of CAS members.Can J Anaesth. 2005 Aug-Sep;52(7):675-9. doi: 10.1007/BF03016552. Can J Anaesth. 2005. PMID: 16103378
-
What laboratory tests are required for ambulatory surgery?Adv Surg. 2013;47:81-98. doi: 10.1016/j.yasu.2013.02.005. Adv Surg. 2013. PMID: 24298845 Review.
-
Preoperative Blood Tests Conducted Before Low-Risk Surgery in Japan: A Retrospective Observational Study Using a Nationwide Insurance Claims Database.Anesth Analg. 2018 May;126(5):1633-1640. doi: 10.1213/ANE.0000000000002734. Anesth Analg. 2018. PMID: 29256933
-
Preoperative testing before noncardiac surgery: guidelines and recommendations.Am Fam Physician. 2013 Mar 15;87(6):414-8. Am Fam Physician. 2013. PMID: 23547574 Review.
Cited by
-
Frequency and costs of low-value preoperative tests for patients undergoing low-risk procedures in the veterans health administration.Perioper Med (Lond). 2022 Sep 13;11(1):33. doi: 10.1186/s13741-022-00265-0. Perioper Med (Lond). 2022. PMID: 36096937 Free PMC article.
-
Variability and Costs of Low-Value Preoperative Testing for Carpal Tunnel Release Surgery.Anesth Analg. 2019 Sep;129(3):804-811. doi: 10.1213/ANE.0000000000004291. Anesth Analg. 2019. PMID: 31425223 Free PMC article.
-
An Economic Evaluation of the Preoperative Investigations for Elective Surgical Patients at a Caribbean Tertiary Care Teaching Hospital.Cureus. 2023 Jan 9;15(1):e33528. doi: 10.7759/cureus.33528. eCollection 2023 Jan. Cureus. 2023. PMID: 36779119 Free PMC article.
-
Value-based preoperative assessment in a large academic hospital.J Anesth Analg Crit Care. 2024 Jul 8;4(1):42. doi: 10.1186/s44158-024-00161-7. J Anesth Analg Crit Care. 2024. PMID: 38978057 Free PMC article.
-
Systematic preoperative tests prescription in elective surgery: it's high time to appraise!Tunis Med. 2022 juillet;100(7):541-546. Tunis Med. 2022. PMID: 36571743 Free PMC article. English.
References
-
- Brown SR, Brown J. Why do physicians order unnecessary preoperative tests? A qualitative study. Fam Med. 2011;43(5):338–343. - PubMed
-
- Committee on Standards and Practice Parameters. Apfelbaum JL, Connis RT, Nickinovich DG, American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Pasternak LR, et al. Practice advisory for preanesthesia evaluation: an updated report by the American Society of Anesthesiologists Task Force on preanesthesia evaluation. Anesthesiology. 2012;116(3):522–538. doi: 10.1097/ALN.0b013e31823c1067. - DOI - PubMed
-
- Czoski-Murray C, Lloyd JM, McCabe C, Claxton K, Oluboyede Y, Roberts J, et al. What is the value of routinely testing full blood count, electrolytes and urea, and pulmonary function test before elective surgery in patients with no apparent clinical indication and in subgroups of patients with common comorbidities: a systematic review of the clinical and cost-effective literature. Health Technol Assess. 2012;16(50):1–159. doi: 10.3310/hta16500. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
