

Epidemiology and Risk Factors for Echinocandin Nonsusceptible Candida glabrata Bloodstream Infections: Data From a Large Multisite Population-Based Candidemia Surveillance Program, 2008-2014
- PMID: 26677456
- PMCID: PMC4677623
- DOI: 10.1093/ofid/ofv163
Epidemiology and Risk Factors for Echinocandin Nonsusceptible Candida glabrata Bloodstream Infections: Data From a Large Multisite Population-Based Candidemia Surveillance Program, 2008-2014
Abstract
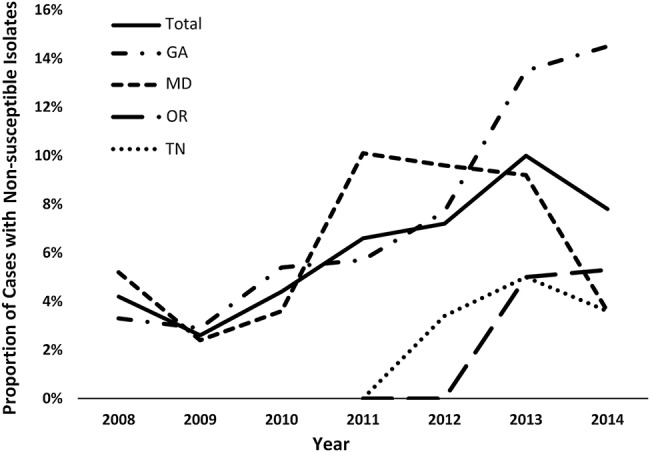
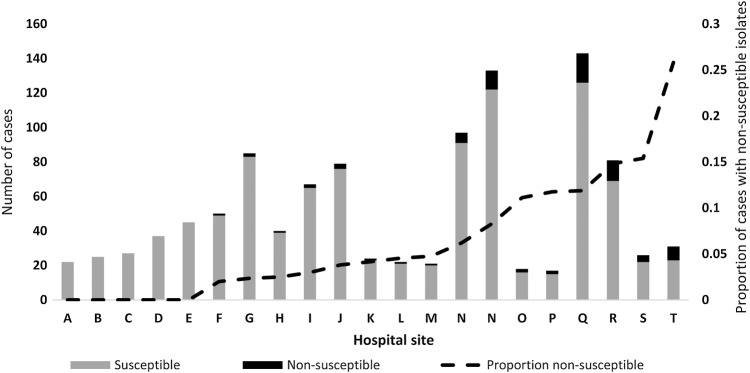
Background. Echinocandins are first-line treatment for Candida glabrata candidemia. Echinocandin resistance is concerning due to limited remaining treatment options. We used data from a multisite, population-based surveillance program to describe the epidemiology and risk factors for echinocandin nonsusceptible (NS) C glabrata candidemia. Methods. The Centers for Disease Control and Prevention's Emerging Infections Program conducts population-based laboratory surveillance for candidemia in 4 metropolitan areas (7.9 million persons; 80 hospitals). We identified C glabrata cases occurring during 2008-2014; medical records of cases were reviewed, and C glabrata isolates underwent broth microdilution antifungal susceptibility testing. We defined echinocandin-NS C glabrata (intermediate or resistant) based on 2012 Clinical and Laboratory Standards Institute minimum inhibitory concentration breakpoints. Independent risk factors for NS C glabrata were determined by stepwise logistic regression. Results. Of 1385 C glabrata cases, 83 (6.0%) had NS isolates (19 intermediate and 64 resistant); the proportion of NS isolates rose from 4.2% in 2008 to 7.8% in 2014 (P < .001). The proportion of NS isolates at each hospital ranged from 0% to 25.8%; 3 large, academic hospitals accounted for almost half of all NS isolates. In multivariate analysis, prior echinocandin exposure (adjusted odds ratio [aOR], 5.3; 95% CI, 2.6-1.2), previous candidemia episode (aOR, 2.5; 95% CI, 1.2-5.1), hospitalization in the last 90 days (aOR, 1.9; 95% CI, 1.0-3.5, and fluconazole resistance [aOR, 3.6; 95% CI, 2.0-6.4]) were significantly associated with NS C glabrata. Fifty-nine percent of NS C glabrata cases had no known prior echinocandin exposure. Conclusion. The proportion of NS C glabrata isolates rose significantly during 2008-2014, and NS C glabrata frequency differed across hospitals. In addition to acquired resistance resulting from prior drug exposure, occurrence of NS C glabrata without prior echinocandin exposure suggests possible transmission of resistant organisms.
Keywords: Candida glabrata; Candidemia; echinocandin resistance; epidemiology; risk factors; transmission of drug resistance.
Figures
References
-
- Kanafani ZA, Perfect JR. Antimicrobial resistance: resistance to antifungal agents: mechanisms and clinical impact. Clin Infect Dis 2008; 46:120–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
