

Asthma Controller Medication Adherence, Risk of Exacerbation, and Use of Rescue Agents Among Texas Medicaid Patients with Persistent Asthma
- PMID: 26679962
- PMCID: PMC10401995
- DOI: 10.18553/jmcp.2015.21.12.1124
Asthma Controller Medication Adherence, Risk of Exacerbation, and Use of Rescue Agents Among Texas Medicaid Patients with Persistent Asthma
Abstract
Background: Adherence to asthma long-term controller medications is one of the key drivers to improve asthma management among patients with persistent asthma. While suboptimal use of controller medications has been found to be associated with more frequent use of oral corticosteroids (OCS), few studies exist regarding the relationship between adherence to controller therapy and the use of short-acting beta2-agonists (SABAs). A better understanding of the association between adherence to asthma controller agents and use of reliever medications will help health care providers and decision makers enhance asthma management.
Objective: To determine if there is a relationship between asthma controller adherence, risk of exacerbation requiring OCS, and use of asthma rescue agents.
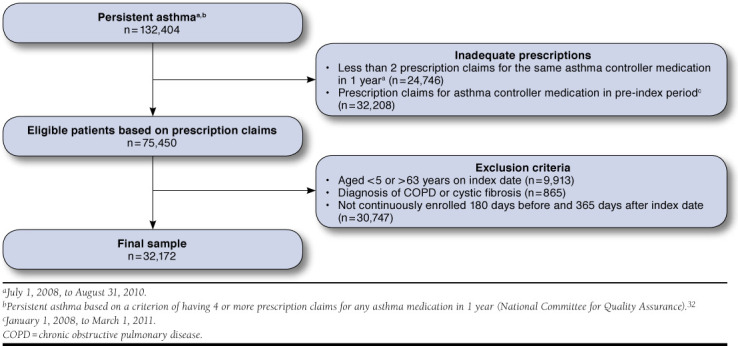
Methods: Texas Medicaid claims data from January 1, 2008, to August 31, 2011, were retrospectively analyzed. Continuously enrolled patients aged 5-63 years with a primary diagnosis of asthma (ICD-9-CM code 493) and with 4 or more prescription claims for any asthma medication in 1 year (persistent asthma) were included. The index date was the date of the first asthma controller prescription, and patients were followed for 1 year. The primary outcome variables were SABA (dichotomous: less than 6 vs. ≥ 6) and OCS (continuous) use. The primary independent variable was adherence (proportion of days covered [PDC]) to asthma long-term controller medications. Covariates included demographics and nonstudy medication utilization. Multivariate logistic and linear regression analyses were employed to address the study objective.
Results: The study sample (n = 32,172) was aged 15.0 ± 14.5 years, and adherence to controller therapy was 32.2% ± 19.7%. The mean number of SABA claims was 3.7 ± 3.1, with most patients having 1-5 claims (73.2%), whereas 19.4% had ≥ 6 SABA claims. The mean number of OCS claims was 1.0 ± 1.4. Adherent (PDC ≥ 50%) patients were 96.7% (OR = 1.967; 95% CI = 1.826-2.120) more likely to have ≥ 6 SABA claims when compared with nonadherent (PDC less than 50%) patients (P less than 0.001). As for OCS use, adherent patients had 0.11 fewer claims compared with nonadherent patients (P less than 0.001). Importantly, patients with ≥ 6 SABA claims had 0.7 more OCS claims compared with patients with less than 6 claims for SABA (P less than 0.001). The odds of having ≥ 6 SABA claims were higher for concurrent dual therapy users, older age, males, African Americans and higher number of nonstudy medications (P less than 0.001). Dual therapy users, younger age, Hispanic ethnicity, and higher number of nonstudy medications were associated with an increase in OCS use (P less than 0.005).
Conclusions: Adherence to long-term controller medications was suboptimal among patients with asthma. Adherent patients had fewer OCS claims, indicating that adherence to controller therapy is critical in preventing asthma exacerbations requiring OCS use. Although there was a positive relationship between adherence to long-term controller medication and SABA use, increased SABA use served as a predictor of increased OCS use, which indicates poor asthma control. Health care providers should be aware of OCS and SABA use among patients who are both adherent and nonadherent to asthma controller medications.
Conflict of interest statement
The authors report no potential conflicts of interest.
Makhinova and Barner collaborated on the conception of the project, study design, data analysis, and writing the manuscript. Richards and Rascati critically reviewed the study design, data analysis, and results interpretation and contributed to the development and editing of the manuscript.
Figures
Similar articles
-
Adequate levels of adherence with controller medication is associated with increased use of rescue medication in asthmatic children.PLoS One. 2012;7(6):e39130. doi: 10.1371/journal.pone.0039130. Epub 2012 Jun 27. PLoS One. 2012. PMID: 22761728 Free PMC article.
-
Exacerbation burden in patients treated as intermittent or mild-persistent asthma using short-acting β2-agonist rescue.Ann Allergy Asthma Immunol. 2025 May;134(5):539-547.e1. doi: 10.1016/j.anai.2025.02.009. Epub 2025 Feb 24. Ann Allergy Asthma Immunol. 2025. PMID: 40010667
-
Economic Burden of Illness Among Patients with Severe Asthma in a Managed Care Setting.J Manag Care Spec Pharm. 2016 Jul;22(7):848-61. doi: 10.18553/jmcp.2016.22.7.848. J Manag Care Spec Pharm. 2016. PMID: 27348285 Free PMC article.
-
Optimizing asthma care in low-to-middle income countries through multisectoral collaboration: recommendation report of the first Philippine Asthma Assembly.Expert Rev Respir Med. 2024 Dec;18(12):947-962. doi: 10.1080/17476348.2024.2389948. Epub 2024 Dec 10. Expert Rev Respir Med. 2024. PMID: 39655400 Review.
-
Expert Consensus on SABA Use for Asthma Clinical Decision-Making: A Delphi Approach.Curr Allergy Asthma Rep. 2023 Nov;23(11):621-634. doi: 10.1007/s11882-023-01111-z. Epub 2023 Nov 22. Curr Allergy Asthma Rep. 2023. PMID: 37991672 Free PMC article. Review.
Cited by
-
Impact of adherence to treatment with inhaled corticosteroids/long-acting β-agonists on asthma outcomes in the United States.Ther Adv Respir Dis. 2022 Jan-Dec;16:17534666221116997. doi: 10.1177/17534666221116997. Ther Adv Respir Dis. 2022. PMID: 36036456 Free PMC article.
-
Effects of an Asthma Self-Management Support Service Provided by Community Pharmacists: A Systematic Review and Meta-Analysis.J Manag Care Spec Pharm. 2018 Nov;24(11):1184-1196. doi: 10.18553/jmcp.2018.24.11.1184. J Manag Care Spec Pharm. 2018. PMID: 30362920 Free PMC article.
-
Seasonal patterns of Asthma medication fills among diverse populations of the United States.J Asthma. 2018 Jul;55(7):764-770. doi: 10.1080/02770903.2017.1362426. Epub 2017 Sep 7. J Asthma. 2018. PMID: 28881155 Free PMC article.
-
Understanding relationships between asthma medication use and outcomes in a SABINA primary care database study.NPJ Prim Care Respir Med. 2022 Oct 21;32(1):43. doi: 10.1038/s41533-022-00310-x. NPJ Prim Care Respir Med. 2022. PMID: 36270999 Free PMC article.
-
[Association between the use of short-acting bronchodilators and the risk of hospitalization for asthma in a real-life clinical practice population cohort].Aten Primaria. 2020 Nov;52(9):600-607. doi: 10.1016/j.aprim.2020.03.004. Epub 2020 Jun 20. Aten Primaria. 2020. PMID: 32571597 Free PMC article. Spanish.
References
-
- National Center for Health Statistics. National Health Interview Survey (NHIS). 2009 data release. Centers for Disease Control and Prevention. 2010. Page updated December 14, 2012. Available at: http://www.cdc.gov/nchs/nhis/nhis_2009_data_release.htm. Accessed October 14, 2015.
-
- National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the diagnosis and management of asthma. Summary report 2007. NIH Publication Number 08-5846. October 2007. Available at: http://www.nhlbi.nih.gov/files/docs/guidelines/asthsumm.pdf. Accessed October 14, 2015.
-
- Williams LK, Pladevall M, Xi H, et al. . Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with asthma. J Allergy Clin Immunol. 2004;114(6):1288-93. - PubMed
-
- Lasmar L, Camargos P, Champs NS, et al. . Adherence rate to inhaled corticosteroids and their impact on asthma control. Allergy. 2009;64(5):784-89. - PubMed
-
- Williams LK, Joseph CL, Peterson EL, et al. . Patients with asthma who do not fill their inhaled corticosteroids: a study of primary nonadherence. J Allergy Clin Immunol. 2007;120(5):1153-59. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
