

A Real-World Observational Study of Time to Treatment Intensification Among Elderly Patients with Inadequately Controlled Type 2 Diabetes Mellitus
- PMID: 26679967
- PMCID: PMC4760631
- DOI: 10.18553/jmcp.2015.21.12.1184
A Real-World Observational Study of Time to Treatment Intensification Among Elderly Patients with Inadequately Controlled Type 2 Diabetes Mellitus
Abstract
Background: Among elderly patients, the management of type 2 diabetes mellitus (T2DM) is complicated by population heterogeneity and elderly-specific complexities. Few studies have been done to understand treatment intensification among elderly patients failing multiple oral antidiabetic drugs (OADs).
Objective: To examine the association between time to treatment intensification of T2DM and elderly-specific patient complexities.
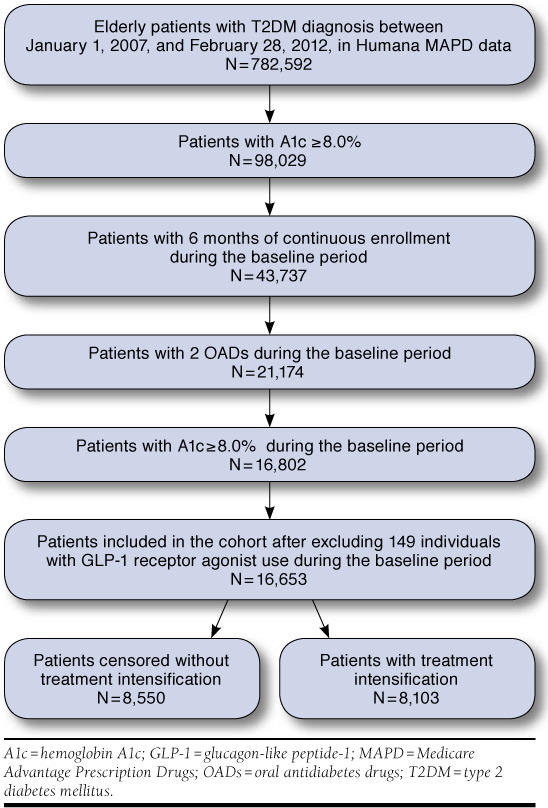
Methods: In this observational, retrospective cohort study, elderly (aged ≥ 65 years) Medicare beneficiaries (n = 16,653) with inadequately controlled T2DM (hemoglobin A1c ≥ 8.0% despite 2 OADs) were included. Based on the consensus statement for diabetes care in elderly patients published by the American Diabetes Association and the American Geriatric Society, elderly-specific patient complexities were defined as the presence or absence of 5 geriatric syndromes: cognitive impairment; depression; falls and fall risk; polypharmacy; and urinary incontinence.
Results: Overall, 48.7% of patients received intensified treatment during follow-up, with median time to intensification 18.5 months (95% CI = 17.7-19.3). Median time to treatment intensification was shorter for elderly patients with T2DM with polypharmacy (16.5 months) and falls and fall risk (12.7 months) versus those without polypharmacy (20.4 months) and no fall risk (18.6 months). Elderly patients with urinary incontinence had a longer median time to treatment intensification (18.6 months) versus those without urinary incontinence (14.6 months). The median time to treatment intensification did not significantly differ by the elderly-specific patient complexities that included cognitive impairment and depression. However, after adjusting for demographic, insurance, clinical characteristics, and health care utilization, we found that only polypharmacy was associated with time to treatment intensification (adjusted hazard ratio, 1.10; 95% CI = 1.04-1.15; P = 0.001).
Conclusions: Less than half of elderly patients with inadequately controlled T2DM received treatment intensification. Elderly-specific patient complexities were not associated with time to treatment intensification, emphasizing a positive effect of the integrated health care delivery model. Emerging health care delivery models that target integrated care may be crucial in providing appropriate treatment for elderly T2DM patients with complex conditions.
Similar articles
-
Influence of Treatment Intensification on A1c in Patients with Suboptimally Controlled Type 2 Diabetes After 2 Oral Antidiabetic Agents.J Manag Care Spec Pharm. 2019 Mar;25(3):314-322. doi: 10.18553/jmcp.2019.25.3.314. J Manag Care Spec Pharm. 2019. PMID: 30816811 Free PMC article.
-
Factors associated with Prolonged Inaction in the hypoglycaemic treatment in people with non-insulin dependent Type 2 Diabetes and elevated glycated haemoglobin: A registry-based cohort study.Prim Care Diabetes. 2017 Oct;11(5):482-489. doi: 10.1016/j.pcd.2017.05.008. Epub 2017 Jun 23. Prim Care Diabetes. 2017. PMID: 28648964
-
Effectiveness and tolerability of second-line treatment with vildagliptin versus other oral drugs for type 2 diabetes in a real-world setting in the Middle East: results from the EDGE study.Vasc Health Risk Manag. 2015 Feb 24;11:149-55. doi: 10.2147/VHRM.S73703. eCollection 2015. Vasc Health Risk Manag. 2015. PMID: 25750538 Free PMC article.
-
Noninsulin treatment of type 2 diabetes mellitus in geriatric patients: a review.Clin Ther. 2011 Dec;33(12):1868-82. doi: 10.1016/j.clinthera.2011.10.020. Epub 2011 Dec 2. Clin Ther. 2011. PMID: 22136979 Review.
-
Type 2 Diabetes Mellitus and the Elderly: An Update on Drugs Used to Treat Glycaemia.Curr Vasc Pharmacol. 2017;15(1):19-29. doi: 10.2174/1570161114666160822154816. Curr Vasc Pharmacol. 2017. PMID: 27550054 Review.
Cited by
-
Overtreatment and Deintensification of Diabetic Therapy among Medicare Beneficiaries.J Gen Intern Med. 2018 Jan;33(1):34-41. doi: 10.1007/s11606-017-4167-y. Epub 2017 Sep 13. J Gen Intern Med. 2018. PMID: 28905179 Free PMC article.
-
Clinical Inertia in Poorly Controlled Type 2 Diabetes Mellitus Patients with Obesity: An Observational Retrospective Study.Diabetes Ther. 2020 Feb;11(2):437-451. doi: 10.1007/s13300-019-00745-5. Epub 2019 Dec 28. Diabetes Ther. 2020. PMID: 31884573 Free PMC article.
-
Efficacy and safety of lixisenatide as add-on therapy to basal insulin in older adults with type 2 diabetes in the GetGoal-O Study.J Diabetes. 2019 Dec;11(12):971-981. doi: 10.1111/1753-0407.12952. Epub 2019 Jun 26. J Diabetes. 2019. PMID: 31094074 Free PMC article. Clinical Trial.
-
The impact of phenotype, ethnicity and genotype on progression of type 2 diabetes mellitus.Endocrinol Diabetes Metab. 2020 Jan 7;3(2):e00108. doi: 10.1002/edm2.108. eCollection 2020 Apr. Endocrinol Diabetes Metab. 2020. PMID: 32318630 Free PMC article. Review.
-
Treatment Intensification in Type 2 Diabetes: A Real-World Study of 2-OAD Regimens, GLP-1 RAs, or Basal Insulin.Diabetes Ther. 2018 Jun;9(3):1169-1184. doi: 10.1007/s13300-018-0429-x. Epub 2018 Apr 19. Diabetes Ther. 2018. PMID: 29675797 Free PMC article.
References
-
- Nathan DM, Buse JB, Davidson MB, et al. . Management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2006;29(8):1963-72. Available at: http://care.diabetesjournals.org/content/29/8/1963.full.pdf+html. Accessed October 20, 2015. - PubMed
-
- Chaudhry SI, Berlowitz DR, Concato J.. Do age and comorbidity affect intensity of pharmacological therapy for poorly controlled diabetes mellitus? J Am Geriatr Soc. 2005;53(7):1214-16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
