

Modality of RRT and Recovery of Kidney Function after AKI in Patients Surviving to Hospital Discharge
- PMID: 26681135
- PMCID: PMC4702218
- DOI: 10.2215/CJN.01290215
Modality of RRT and Recovery of Kidney Function after AKI in Patients Surviving to Hospital Discharge
Abstract
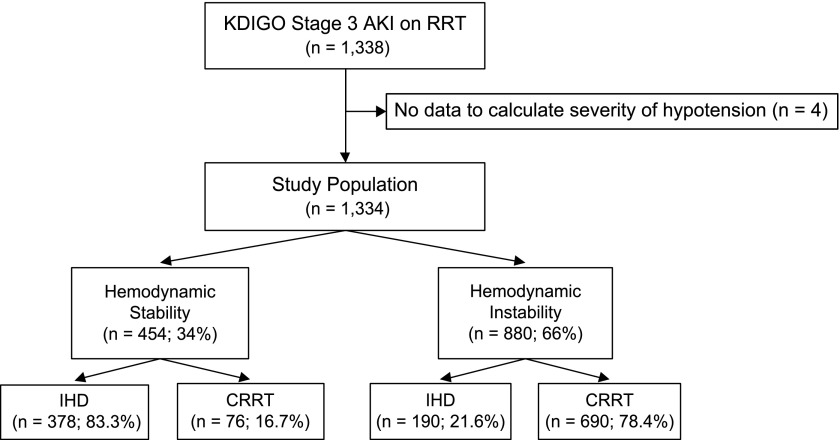
Background and objectives: Observational evidence has suggested that RRT modality may affect recovery after AKI. It is unclear whether initial choice of intermittent hemodialysis or continuous RRT affects renal recovery, survival, or development of ESRD in critically ill patients when modality choice is made primarily on hemodynamics.
Design, setting, participants, & measurements: We performed a retrospective cohort study examining adults (≥18 years old) admitted to intensive care units from 2000 to 2008 who received RRT for AKI and survived to hospital discharge or 90 days. We analyzed renal recovery (alive and not requiring RRT) and reasons for nonrecovery (death or ESRD) at 90 and 365 days. Conditional multivariable logistic regression was used to assess differences in renal recovery at 90 and 365 days between continuous RRT and intermittent hemodialysis. Models were stratified by propensity for continuous RRT and adjusted for age and reference creatinine.
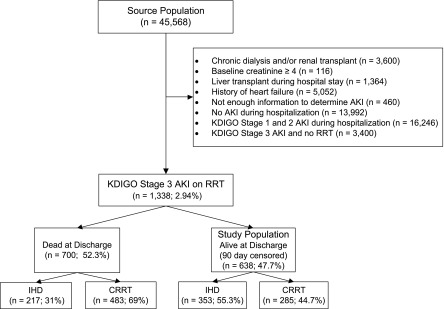
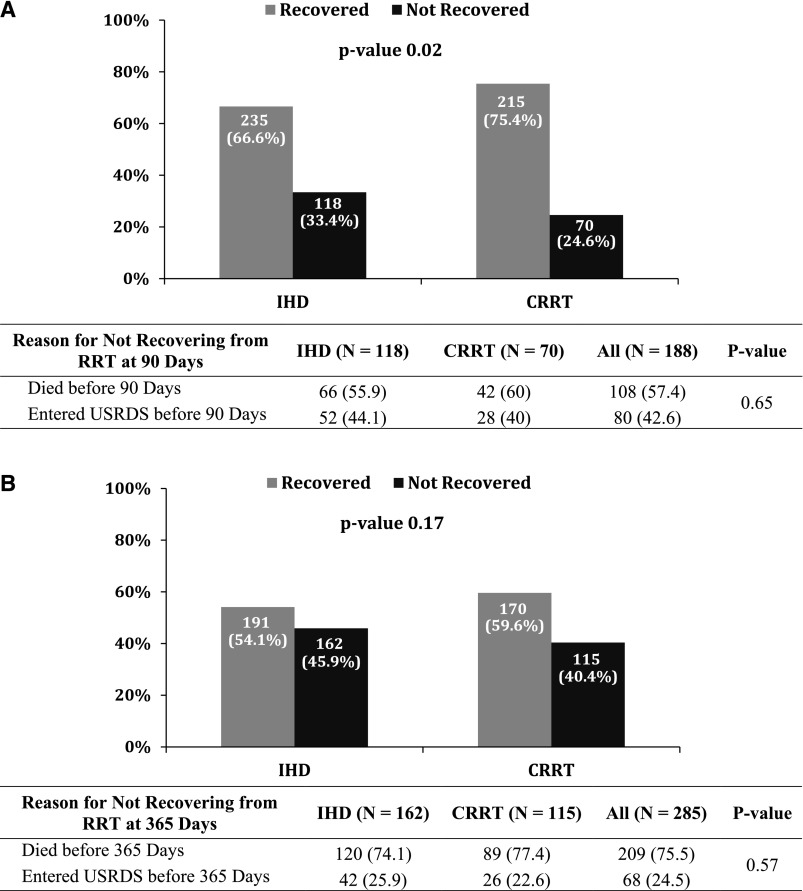
Results: Of 4738 patients with Kidney Disease Improving Global Outcomes stage 3 AKI, 1338 (28.2%) received RRT, and 638 (47.7%) survived to hospital discharge (353 intermittent hemodialysis and 285 continuous RRT). Recovery from AKI was lower for intermittent hemodialysis versus continuous RRT at 90 days (66.6% intermittent hemodialysis versus 75.4% continuous RRT; P=0.02) but similar at 365 days (54.1% intermittent hemodialysis versus 59.6% continuous RRT; P=0.17). In multivariable analysis, there was no difference in odds of recovery at 90 or 365 days for patients initially treated with continuous RRT versus intermittent hemodialysis (90 days: odds ratio, 1.19; 95% confidence interval, 0.91 to 1.55; P=0.20; 365 days: odds ratio, 0.93; 95% confidence interval, 0.72 to 1.2; P=0.55).
Conclusions: We found no significant difference in hazards for nonrecovery or reasons for nonrecovery (mortality or ESRD) with intermittent hemodialysis versus continuous RRT. These results suggest that, when initial RRT modality is chosen primarily on hemodynamics, renal recovery and clinical outcomes in survivors are similar between intermittent hemodialysis and continuous RRT.
Keywords: Hemodialysis; acute kidney injury; cohort studies; critical illness; hemodynamics; humans; intensive care units; kidney failure, chronic; renal replacement therapy.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Schneider AG, Bellomo R, Bagshaw SM, Glassford NJ, Lo S, Jun M, Cass A, Gallagher M: Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: A systematic review and meta-analysis. Intensive Care Med 39: 987–997, 2013 - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators : Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 294: 813–818, 2005 - PubMed
-
- Hoste EAJ, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, Honoré PM, Joannes-Boyau O, Joannidis M, Korhonen AM, Lavrentieva A, Mehta RL, Palevsky P, Roessler E, Ronco C, Uchino S, Vazquez JA, Vidal Andrade E, Webb S, Kellum JA: Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med 41: 1411–1423, 2015 - PubMed
-
- Wald R, Shariff SZ, Adhikari NKJ, Bagshaw SM, Burns KEA, Friedrich JO, Garg AX, Harel Z, Kitchlu A, Ray JG: The association between renal replacement therapy modality and long-term outcomes among critically ill adults with acute kidney injury: A retrospective cohort study. Crit Care Med 42: 868–877, 2014 - PubMed
-
- Bellomo R, Baldwin I, Fealy N: Prolonged intermittent renal replacement therapy in the intensive care unit. Crit Care Resusc 4: 281–290, 2002 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
