

Stereotactic Radiosurgery for Renal Cancer Brain Metastasis: Prognostic Factors and the Role of Whole-Brain Radiation and Surgical Resection
- PMID: 26681942
- PMCID: PMC4668321
- DOI: 10.1155/2015/636918
Stereotactic Radiosurgery for Renal Cancer Brain Metastasis: Prognostic Factors and the Role of Whole-Brain Radiation and Surgical Resection
Abstract
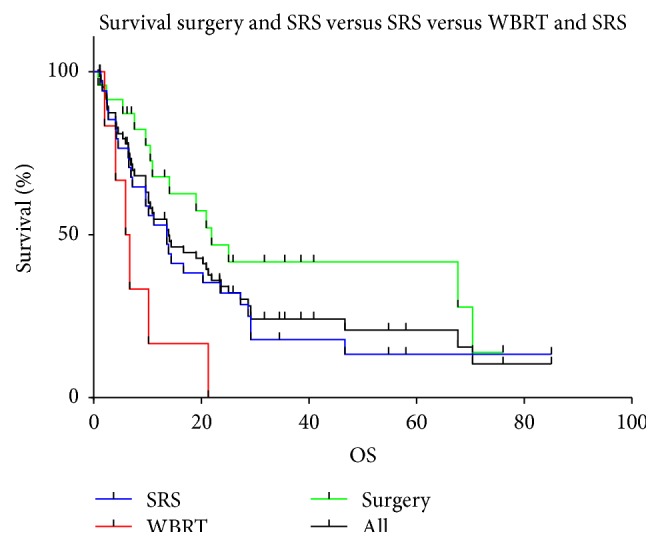
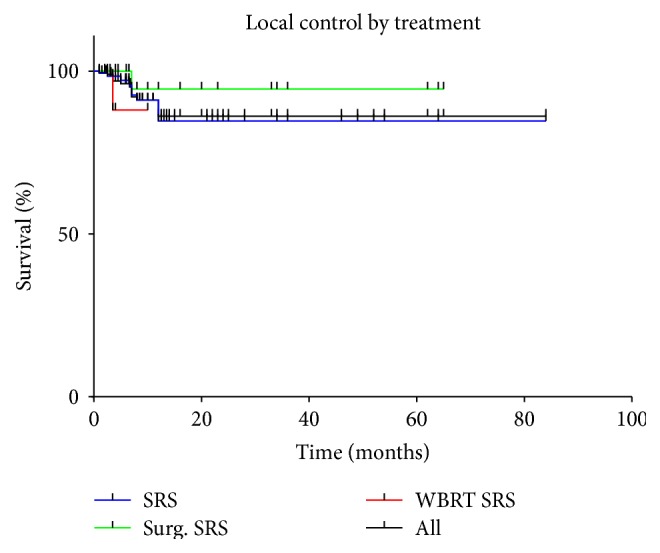
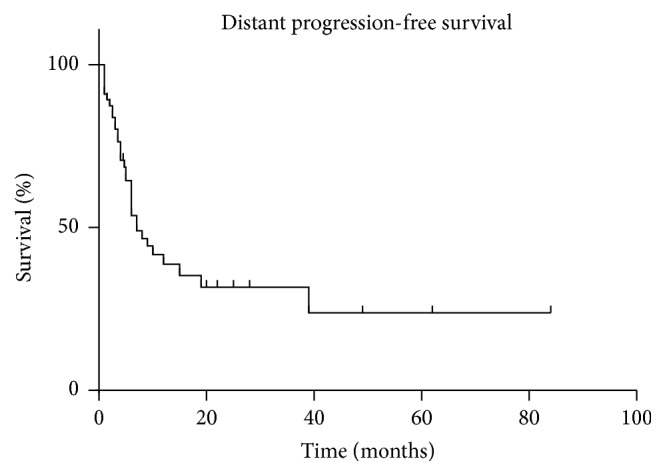
Background. Renal cell carcinoma is a frequent source of brain metastasis. We present our consecutive series of patients treated with Stereotactic Radiosurgery (SRS) and analyse prognostic factors and the interplay of WBRT and surgical resection. Methods. This is a retrospective study of 66 patients with 207 lesions treated with the Cyberknife radiosurgery system in our institution. The patients were followed up with imaging and clinical examination 1 month and 2-3 months thereafter for the brain metastasis. Patient, treatment, and outcomes characteristics were analysed. Results. 51 male (77.3%) and 15 female (22.7%) patients, with a mean age of 58.9 years (range of 31-85 years) and a median Karnofsky Performance Status (KPS) of 90 (range of 60-100), were included in the study. The overall survival was 13.9 months, 21.9 months, and 5.9 months for the patients treated with SRS only, additional surgery, and WBRT, respectively. The actuarial 1-year Local Control rates were 84%, 94%, and 88% for SRS only, for surgery and SRS, and for WBRT and additional SRS, respectively. Conclusions. Stereotactic radiosurgery is a safe and effective treatment option in patients with brain metastases from RCC. In case of a limited number of brain metastases, surgery and SRS might be appropriate.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
