

HIV, antiretroviral treatment, hypertension, and stroke in Malawian adults: A case-control study
- PMID: 26683649
- PMCID: PMC4776088
- DOI: 10.1212/WNL.0000000000002278
HIV, antiretroviral treatment, hypertension, and stroke in Malawian adults: A case-control study
Abstract
Objective: To investigate HIV, its treatment, and hypertension as stroke risk factors in Malawian adults.
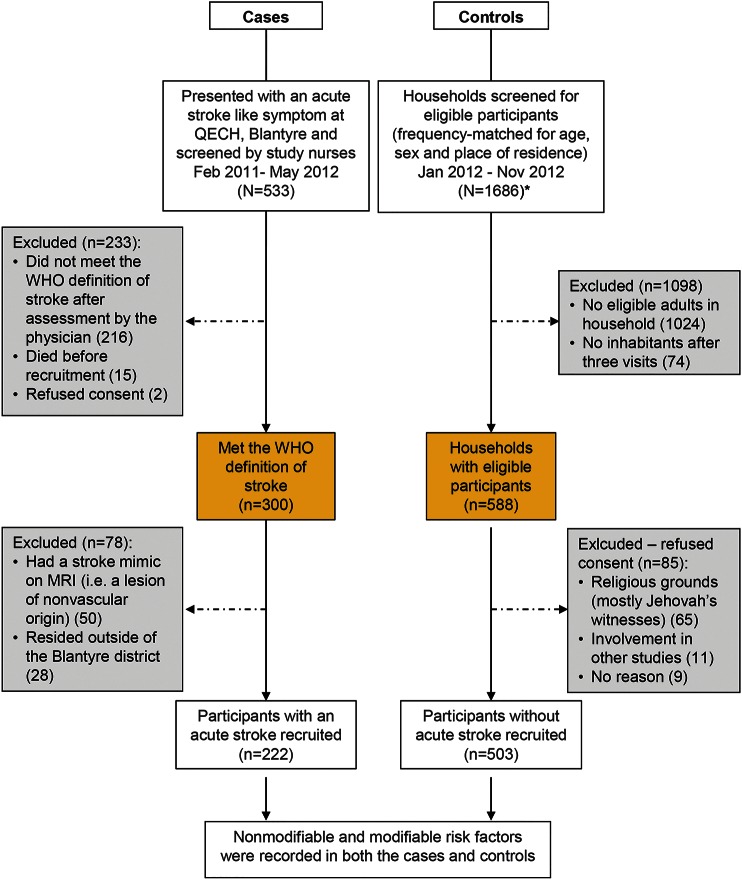
Methods: We performed a case-control study of 222 adults with acute stroke, confirmed by MRI in 86%, and 503 population controls, frequency-matched for age, sex, and place of residence, using Global Positioning System for random selection. Multivariate logistic regression models were used for case-control comparisons.
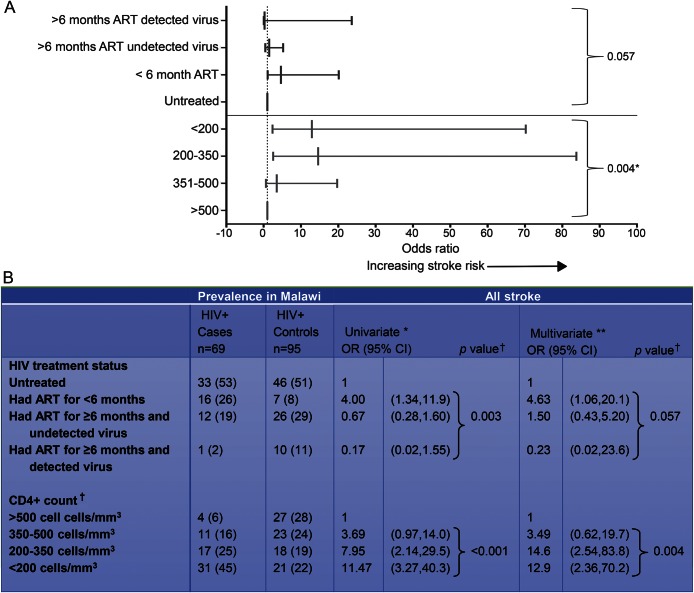
Results: HIV infection (population attributable fraction [PAF] 15%) and hypertension (PAF 46%) were strongly linked to stroke. HIV was the predominant risk factor for young stroke (≤45 years), with a prevalence of 67% and an adjusted odds ratio (aOR) (95% confidence interval) of 5.57 (2.43-12.8) (PAF 42%). There was an increased risk of a stroke in patients with untreated HIV infection (aOR 4.48 [2.44-8.24], p < 0.001), but the highest risk was in the first 6 months after starting antiretroviral therapy (ART) (aOR 15.6 [4.21-46.6], p < 0.001); this group had a lower median CD4(+) T-lymphocyte count (92 vs 375 cells/mm(3), p = 0.004). In older participants (HIV prevalence 17%), HIV was associated with stroke, but with a lower PAF than hypertension (5% vs 68%). There was no interaction between HIV and hypertension on stroke risk.
Conclusions: In a population with high HIV prevalence, where stroke incidence is increasing, we have shown that HIV is an important risk factor. Early ART use in immunosuppressed patients poses an additional and potentially treatable stroke risk. Immune reconstitution inflammatory syndrome may be contributing to the disease mechanisms.
© 2015 American Academy of Neurology.
Figures
Comment in
-
The merging burden of HIV infection and stroke in the developing world.Neurology. 2016 Jan 26;86(4):316-7. doi: 10.1212/WNL.0000000000002275. Epub 2015 Dec 18. Neurology. 2016. PMID: 26683640 No abstract available.
References
-
- Friis-Moller N, Weber R, Reiss P, et al. Cardiovascular disease risk factors in HIV patients: association with antiretroviral therapy: results from the DAD study. AIDS 2003;17:1179–1193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials