

INTERMACS profiles and modifiers: Heterogeneity of patient classification and the impact of modifiers on predicting patient outcome
- PMID: 26683809
- PMCID: PMC5600320
- DOI: 10.1016/j.healun.2015.10.037
INTERMACS profiles and modifiers: Heterogeneity of patient classification and the impact of modifiers on predicting patient outcome
Abstract
Background: Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) patient profiles and modifiers are descriptors of patient illness severity before durable ventricular assist device implantation. It is unknown how individual U.S. institutions and practitioners assign profiles and if modifiers improve on risk discrimination.
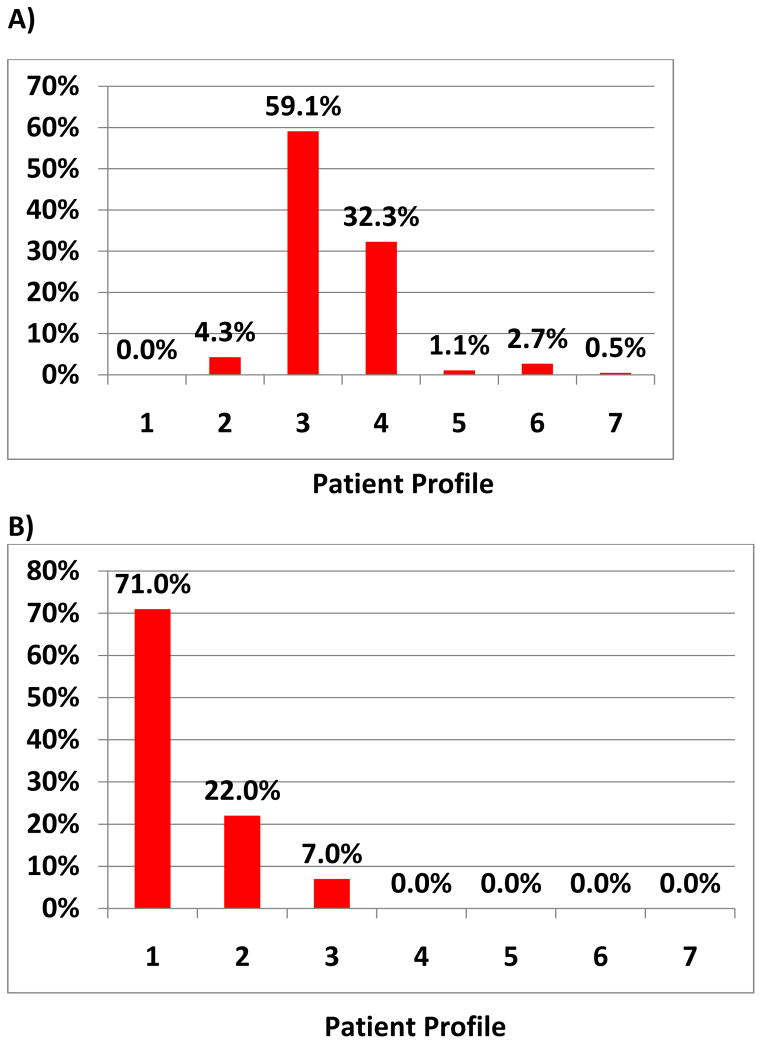
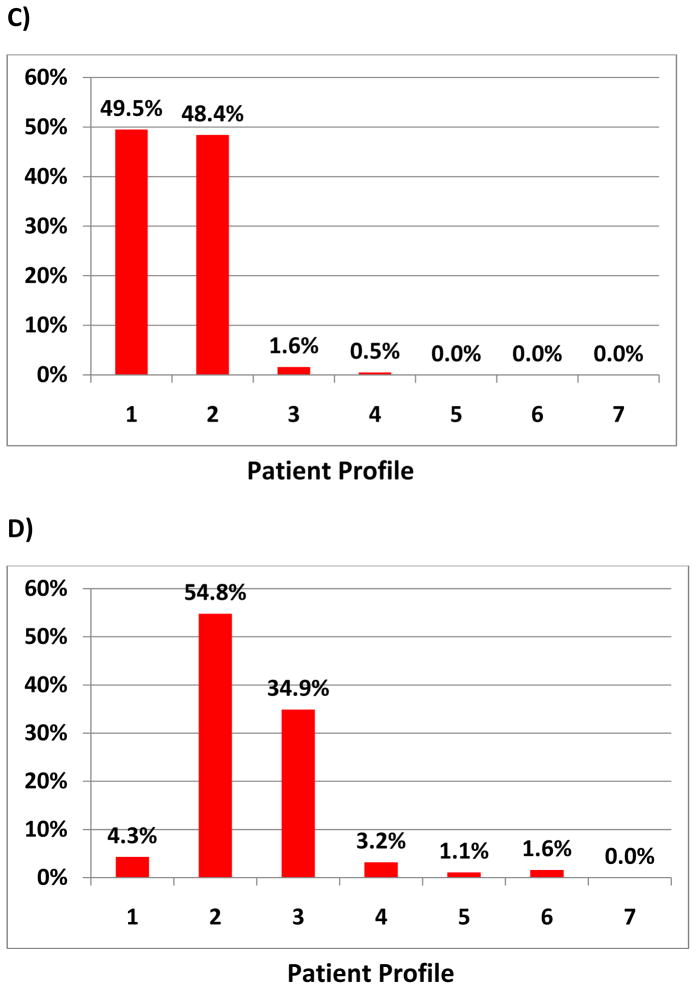
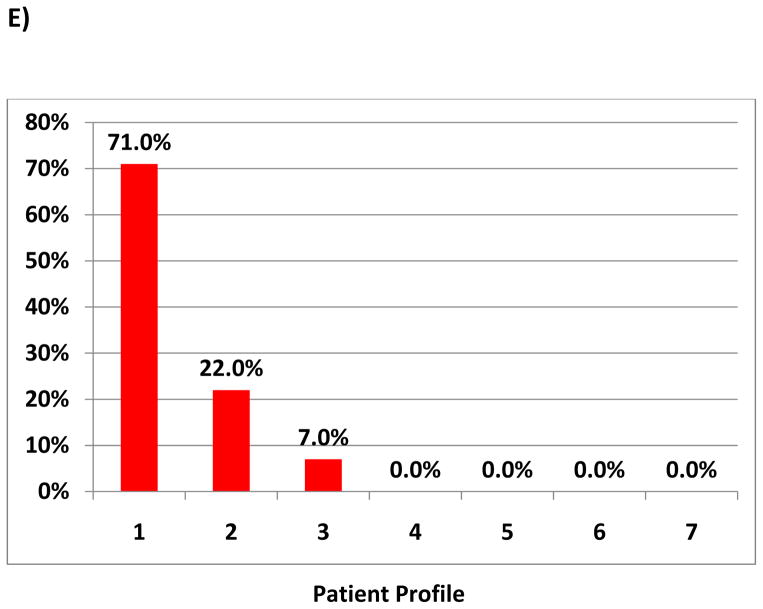
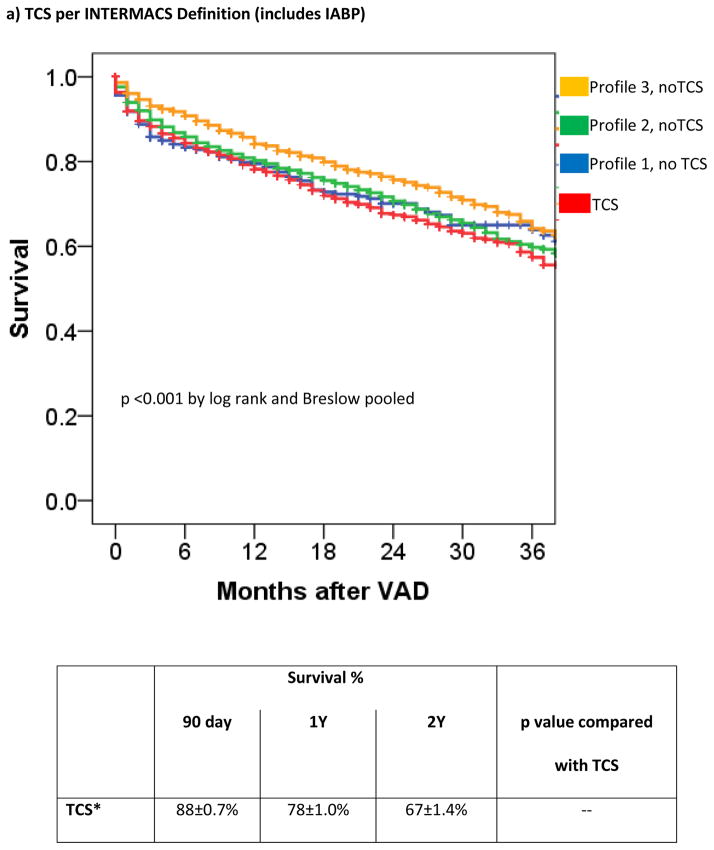
Methods: Respondents (n = 212) to a web-based survey answered questions about the INTERMACS profile assignment process in their institution. For 5 hypothetical clinical scenarios, respondents assigned the best profile. The INTERMACS registry (2009-2014) was queried, and hazard ratio (HR) (95% confidence interval [CI]) for mortality between profiles as well as based on the presence of temporary circulatory support (TCS), frequent flyer (FF), or arrhythmia modifiers was calculated.
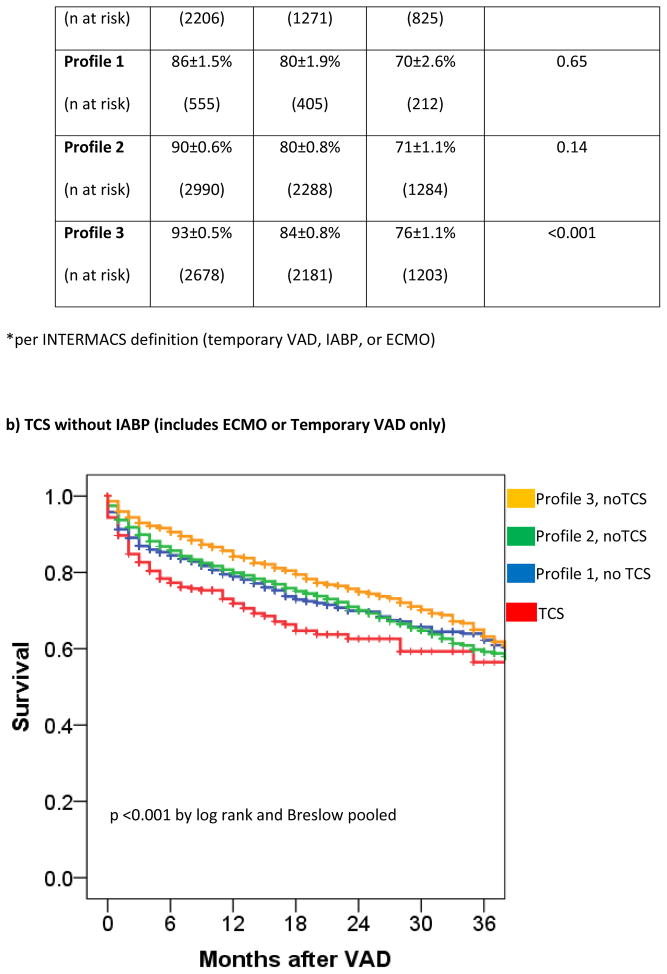
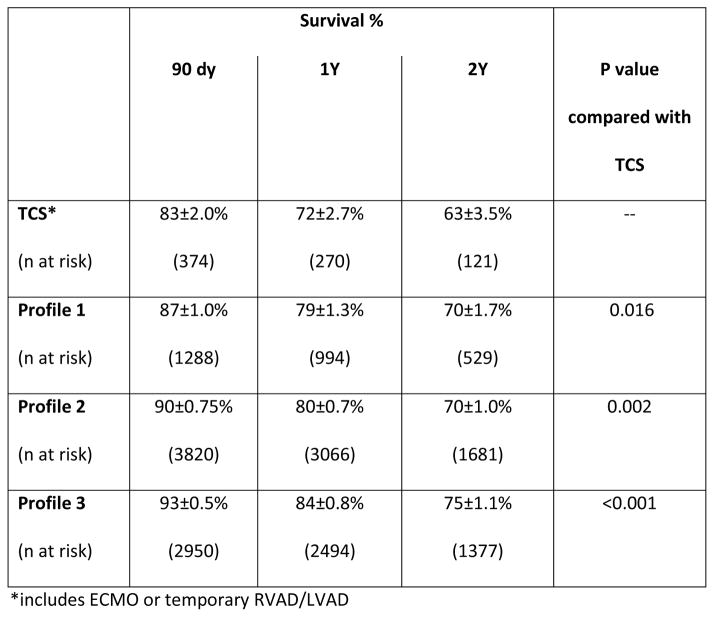
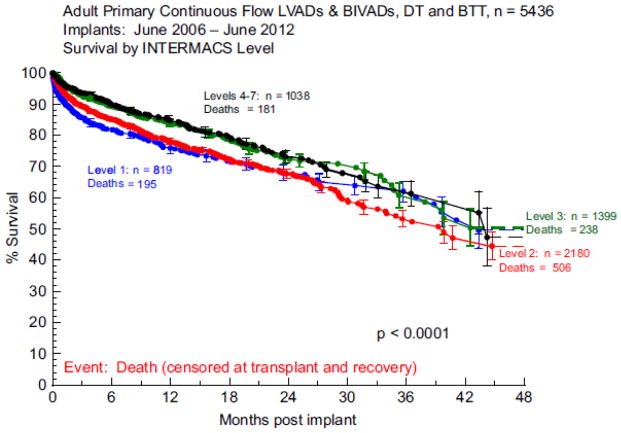
Results: Respondents included 131 (62%) cardiologists, 30 (14%) surgeons, and 51 (24%) physician extenders/coordinators. Institutional INTERMACS profile assignment was variable (63% assigned by cardiologists/surgeons; 10% by research coordinators; 27% by physician extenders). Profile assignments in hypothetical patient scenarios were heterogeneous, especially for contiguous profiles. The 1-year survivals for Profiles 1, 2, and 3 were 77 ± 1.2%, 80 ± 0.7%, and 84 ± 0.7% (p < 0.001). Although Profile 1 patients had worse adjusted survival than Profile 3 patients (p = 0.001), survival for Profile 1 patients vs Profile 2 patients was similar (adjusted HR = 1.01 [95% CI = 0.88-1.12]). The TCS (adjusted HR = 1.1 [95% CI = 0.94-1.2]) and arrhythmia (adjusted HR = 1.1 [95% CI = 0.97-1.2]) modifiers were not predictive of mortality, but the FF modifier was (HR = 1.3 [95% CI = 1.02-1.63]).
Conclusions: Substantial heterogeneity exists in the process and assignment of INTERMACS profiles. This heterogeneity could affect mortality estimates used for risk stratification. Only the FF modifier appears to improve risk discrimination beyond that of known risk factors. Adding objective descriptors may reduce profile heterogeneity.
Keywords: LVAD; mortality; prediction; temporary circulatory support.
Copyright © 2016 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Stevenson LW, Pagani FD, Young JB, et al. INTERMACS Profiles of advanced heart failure: The current picture. J Heart Lung Transplant. 2009;28:535–41. - PubMed
-
- Kirklin JK, Naftel DC, Pagani FD, et al. Sixth INTERMACS annual report: A 10,000-patient database. J Heart Lung Transplant. 2014;33:555–564. - PubMed
-
- Boyle AJ, Ascheim DD, Russo MJ, et al. Clinical outcomes for continuous-flow left ventricular assist device patients stratified by pre-operative INTERMACS classification. J Heart Lung Transplant. 2011;30:402–7. - PubMed
-
- INTERMACS Manual of Operations and Procedures. Retrieved from https://www.uab.edu/medicine/intermacs/images/protocol_4.0/Data_Collecti....
-
- Kirklin JK, Naftel DC, Kormos EL, et al. Fifth INTERMACS annual report: Risk factor analysis form more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant. 2013;32:141–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
