

HIV-Related Medical Admissions to a South African District Hospital Remain Frequent Despite Effective Antiretroviral Therapy Scale-Up
- PMID: 26683950
- PMCID: PMC5058922
- DOI: 10.1097/MD.0000000000002269
HIV-Related Medical Admissions to a South African District Hospital Remain Frequent Despite Effective Antiretroviral Therapy Scale-Up
Abstract
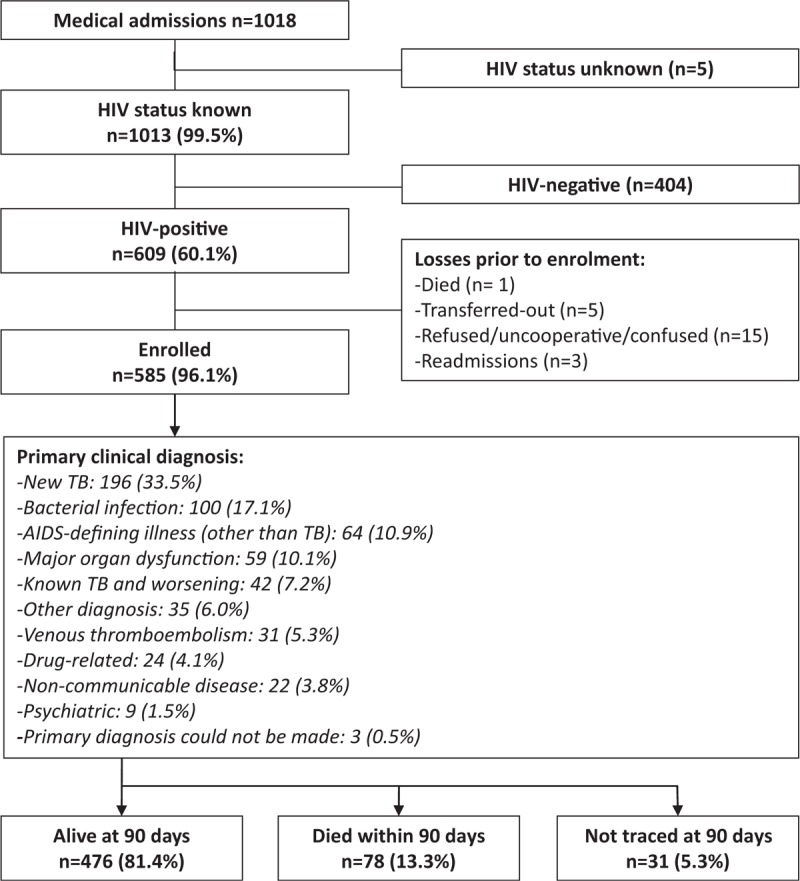
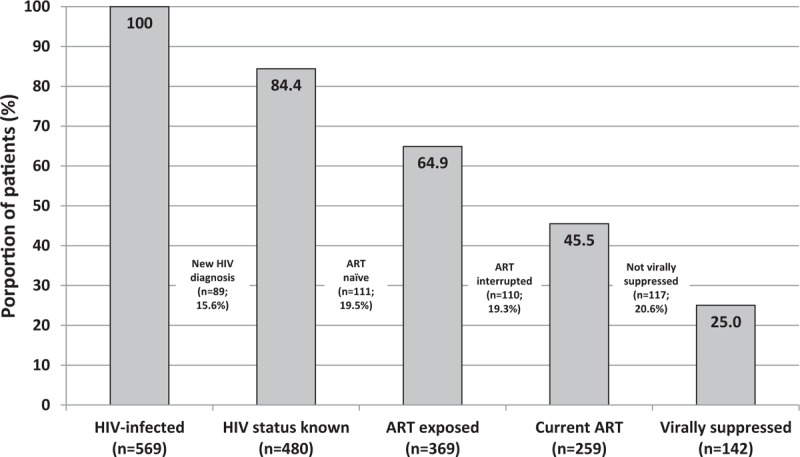
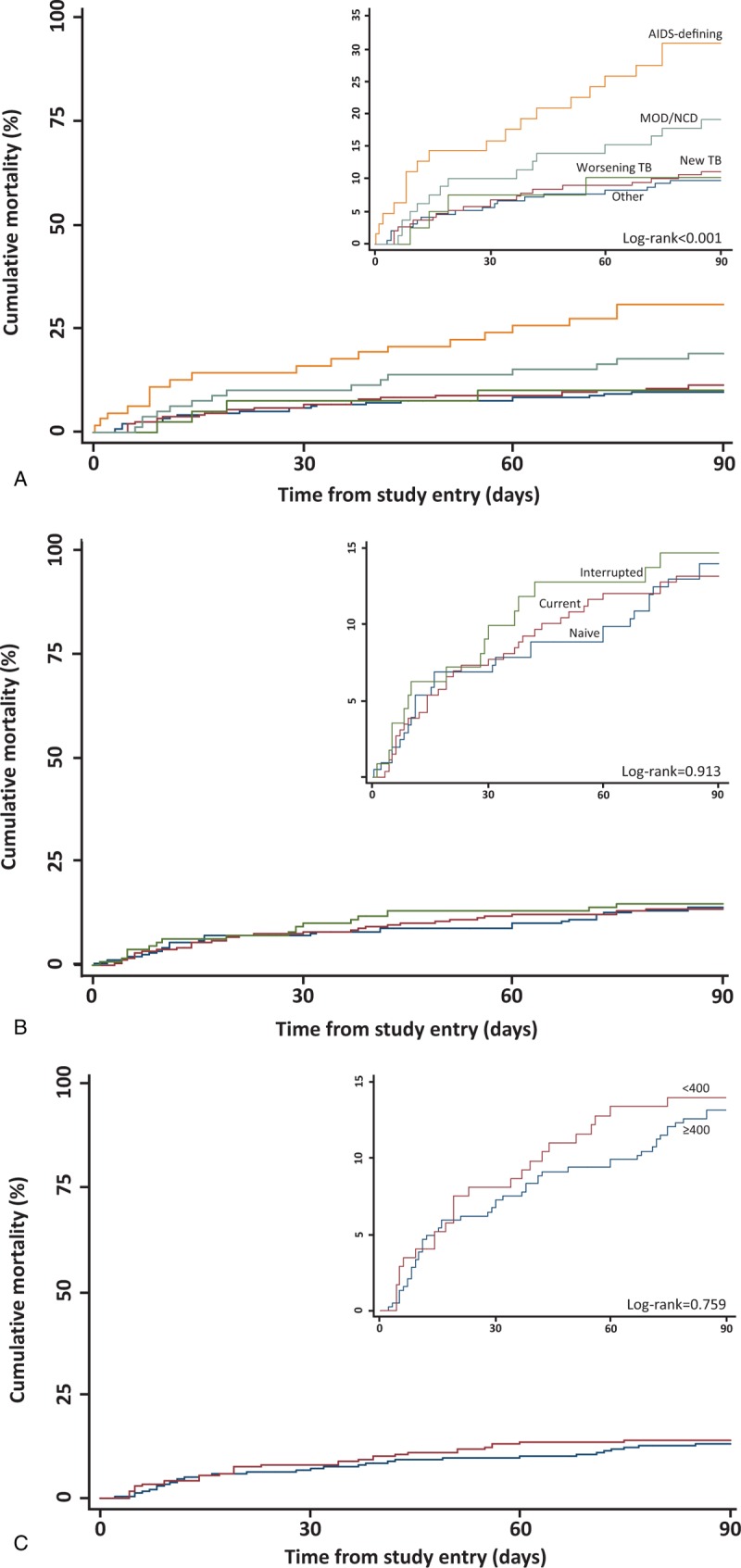
The public sector scale-up of antiretroviral therapy (ART) in South Africa commenced in 2004. We aimed to describe the hospital-level disease burden and factors contributing to morbidity and mortality among hospitalized HIV-positive patients in the era of widespread ART availability. Between June 2012 and October 2013, unselected patients admitted to medical wards at a public sector district hospital in Cape Town were enrolled in this cross-sectional study with prospective follow-up. HIV testing was systematically offered and HIV-infected patients were systematically screened for TB. The spectrum of admission diagnoses among HIV-positive patients was documented, vital status at 90 and 180 days ascertained and factors independently associated with death determined. Among 1018 medical admissions, HIV status was ascertained in 99.5%: 60.1% (n = 609) were HIV-positive and 96.1% (n = 585) were enrolled. Of these, 84.4% were aware of their HIV-positive status before admission. ART status was naive in 35.7%, current in 45.0%, and interrupted in 19.3%. The most frequent primary clinical diagnoses were newly diagnosed TB (n = 196, 33.5%), other bacterial infection (n = 100, 17.1%), and acquired immunodeficiency syndrome (AIDS)-defining illnesses other than TB (n = 64, 10.9%). By 90 days follow-up, 175 (29.9%) required readmission and 78 (13.3%) died. Commonest causes of death were TB (37.2%) and other AIDS-defining illnesses (24.4%). Independent predictors of mortality were AIDS-defining illnesses other than TB, low hemoglobin, and impaired renal function. HIV still accounts for nearly two-thirds of medical admissions in this South African hospital and is associated with high mortality. Strategies to improve linkage to care, ART adherence/retention and TB prevention are key to reducing HIV-related hospitalizations in this setting.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Human Sciences Research Council. South African National HIV Prevalence, Incidence and Behaviour Survey 2012. Cape Town, South Africa: HSRC Press; 2014.
-
- Bekker LG, Venter F, Cohen K, et al. Provision of antiretroviral therapy in South Africa: the nuts and bolts. Antivir Ther 2014; 19 Suppl 3:105–116. - PubMed
-
- Global Update on the Health Sector Response to HIV, 2014. World Health Organization, Geneva, July 2014.
