

A Simple and Portable Algorithm for Identifying Atrial Fibrillation in the Electronic Medical Record
- PMID: 26684516
- PMCID: PMC4706785
- DOI: 10.1016/j.amjcard.2015.10.031
A Simple and Portable Algorithm for Identifying Atrial Fibrillation in the Electronic Medical Record
Abstract
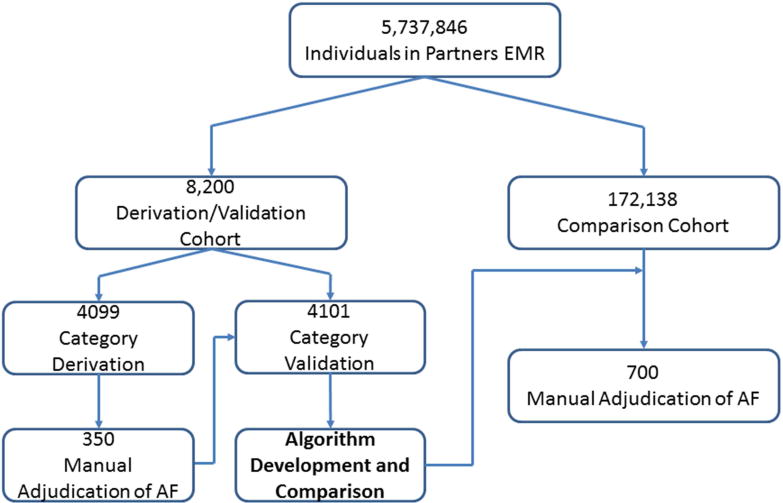
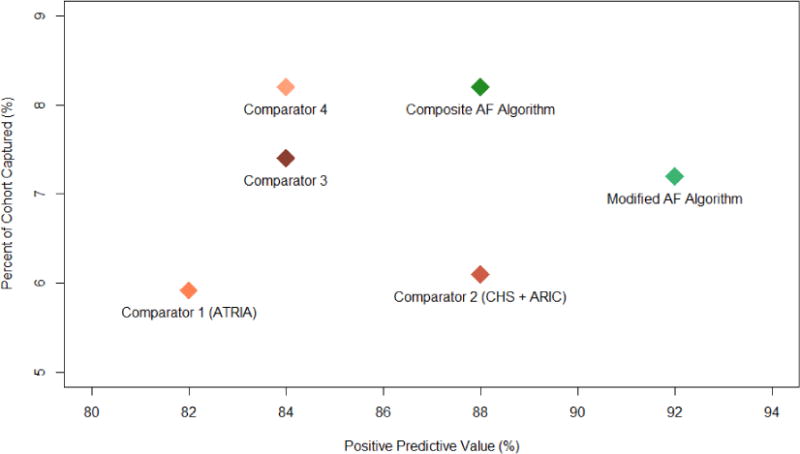
Atrial fibrillation (AF) is common and increases stroke risk and mortality. Many knowledge gaps remain with respect to practice patterns and outcomes. Electronic medical records (EMRs) may serve as powerful research tools if AF status can be properly ascertained. We sought to develop an algorithm for identifying subjects with and without AF in the EMR and compare it to previous methods. Using a hospital network EMR (n = 5,737,846), we randomly selected 8,200 subjects seen at a large academic medical center in January 2014 to derive and validate 7 AF classification schemas (4 cases and 3 controls) to construct a composite AF algorithm. In an independent sample of 172,138 subjects, we compared this algorithm against published AF classification methods. In total, we performed manual adjudication of AF in 700 subjects. Three AF schemas (AF1, AF2, and AF4) achieved positive predictive value (PPV) >0.9. Two control schemas achieved PPV >0.9 (control 1 and control 3). A combination algorithm AF1, AF2, and AF4 (PPV 88%; 8.2% classified) outperformed published classification methods including >1 outpatient International Statistical Classification of Diseases, Ninth Revision code or 1 outpatient code with an electrocardiogram demonstrating AF (PPV 82%; 5.9% classified), ≥ 1 inpatient International Statistical Classification of Diseases, Ninth Revision code or electrocardiogram demonstrating AF (PPV 88%; 6.1% classified), or the intersection of these (PPV 84%; 7.4% classified). When applied simultaneously, the case and control algorithms classified 98.4% of the cohort with zero disagreement. In conclusion, we derived a parsimonious and portable algorithm to identify subjects with and without AF with high sensitivity. If broadly applied, this algorithm can provide optimal power for EMR-based AF research.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Corley SD, Epstein AE, DiMarco JP, Domanski MJ, Geller N, Greene HL, Josephson RA, Kellen JC, Klein RC, Krahn AD, Mickel M, Mitchell LB, Nelson JD, Rosenberg Y, Schron E, Shemanski L, Waldo AL, Wyse DG. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004;109:1509–1513. - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113:359–364. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: a major contributor to stroke in the elderly. The Framingham Study. Arch Intern Med. 1987;147:1561–1564. - PubMed
-
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, Newton-Cheh C, Lubitz SA, Magnani JW, Ellinor PT, Seshadri S, Wolf PA, Vasan RS, Benjamin EJ, Levy D. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–162. - PMC - PubMed
-
- Wilke T, Groth A, Mueller S, Pfannkuche M, Verheyen F, Linder R, Maywald U, Kohlmann T, Feng YS, Breithardt G, Bauersachs R. Oral anticoagulation use by patients with atrial fibrillation in Germany. Adherence to guidelines, causes of anticoagulation under-use and its clinical outcomes, based on claimsdata of 183,448 patients. Thromb Haemost. 2012;107:1053–1065. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
