

Adrenohepatic fusion: Adhesion or invasion in primary virilizant giant adrenal carcinoma? Implications for surgical resection. Two case report and review of the literature
- PMID: 26684865
- PMCID: PMC4701873
- DOI: 10.1016/j.ijscr.2015.10.012
Adrenohepatic fusion: Adhesion or invasion in primary virilizant giant adrenal carcinoma? Implications for surgical resection. Two case report and review of the literature
Abstract
Introduction: Adrenohepatic fusion means union between the adrenal gland and the liver, intermingling its parenchymas. It is not possible to identify this condition by image tests. Its presence implies radical and multidisciplinar approach.
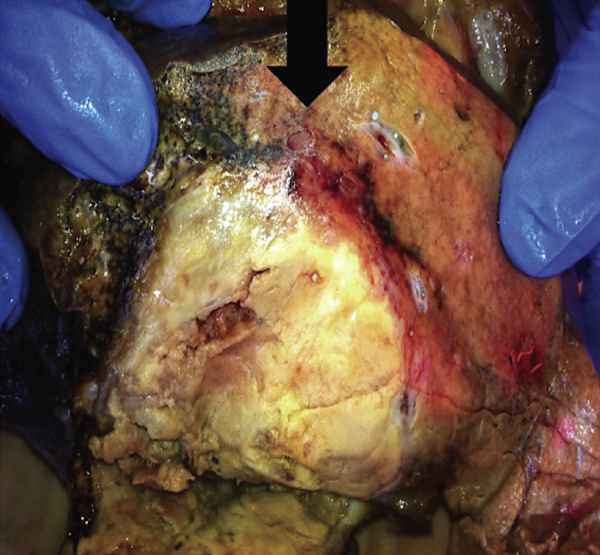
Presentation of cases: We report two female cases of 45 and 50 years old with clinical virilization and palpable mass on the abdominal right upper quadrant corresponding to adrenocortical carcinoma with hepatic fusion. The contrast-enhanced tomography showed an indistinguishable mass involving the liver and the right adrenal gland. In the first case, the patient had a two-time operation, the former removing only the adrenal carcinoma, and the second performing a radical surgery after an early relapse. In the second case, a radical right en bloc adrenohepatectomy was performed. Both cases were pathologically reported as liver-infiltrating adrenal carcinoma. Only in the second case the surgery was radical effective as first intention to treat, with 3 years of disease-free survival.
Discussion: ACC is a rare entity with poor prognosis. The major indicators of malignancy are tumour diameter over 6cm, local invasion or metastasis, secretion of corticosteroids, virilization and hypertension and hypokalaemia. The parenchymal fusion of the adrenal cortical layer can be misdiagnosed as hepatocellular carcinoma with adhesion with the Glisson capsule. AHF in such cases may be misinterpreted during surgery, what may impair its resectability, and therefore the survival. The surgical treatment must be performed en bloc, often using liver vascular control. Postoperative treatment must be offered immediately after surgery.
Conclusion: We report two consecutive rare cases of adrenohepatic fusion in giant right adrenocortical carcinoma, not detectable by imaging, what has important implications for the surgical decision-making. As radical surgery is the best choice to offer a curative treatment, it has to be performed by a multidisciplinary well-assembled team, counting with endocrine and liver surgeons, and transplant surgeons in case of vena cava involvement, in order to maximize the disease-free survival.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures




Similar articles
-
Unusual Techniques for Preserving Surgical and Oncologic Safety in Hepatectomy of Advanced Adrenal Malignancy with Vena Cava and Liver Invasion.Ann Surg Oncol. 2018 Oct;25(11):3324-3325. doi: 10.1245/s10434-018-6657-5. Epub 2018 Jul 17. Ann Surg Oncol. 2018. PMID: 30019302
-
Intrahepatic adrenocortical adenoma arising from adrenohepatic fusion mimicking hepatic malignancy: Two case reports.Medicine (Baltimore). 2019 Jun;98(23):e15901. doi: 10.1097/MD.0000000000015901. Medicine (Baltimore). 2019. PMID: 31169702 Free PMC article.
-
An Interesting Case of Hepatic Adrenocortical Carcinoma.Acta Med Indones. 2018 Jul;50(3):257-259. Acta Med Indones. 2018. PMID: 30333277
-
[Adrenohepatic fusion - an unknown but not uncommon phenomenon of clinical importance].Lakartidningen. 2023 Apr 13;120:23014. Lakartidningen. 2023. PMID: 37052304 Review. Swedish.
-
Direct and indirect imaging features of adrenohepatic fusion.Abdom Radiol (NY). 2016 Feb;41(2):377-83. doi: 10.1007/s00261-015-0573-y. Abdom Radiol (NY). 2016. PMID: 26867924 Review.
Cited by
-
Diagnostic challenges associated with adrenocortical neoplasms arising from adreno-hepatic fusion: a case report of two patients and a literature review.Gland Surg. 2024 Dec 31;13(12):2420-2429. doi: 10.21037/gs-24-367. Epub 2024 Dec 25. Gland Surg. 2024. PMID: 39822371 Free PMC article.
-
Giant Adrenocortical Carcinoma: A Case Report and Review of the Relevant Literature.Am J Case Rep. 2021 Apr 4;22:e928875. doi: 10.12659/AJCR.928875. Am J Case Rep. 2021. PMID: 33813589 Free PMC article.
References
-
- Dolan M., Janovski N. Adreno-hepatic union (adrenal dystopia) Arch. Pathol. 1968;86:22–24. - PubMed
-
- Mihai R., Farndon J. Diagnosis and treatment of adrenal tumors. Surgery. 1996;9:145–153.
-
- Didolkar M., Bescher R., Elias E., Moore R. Natural history of adrenal cortical carcinoma: a clinicopathologic study of 42 patients. Cancer. 1981;47:2153–2161. - PubMed
-
- Derksen J., Nagesser S., Meinders A., Haak H., van-de-Velde C. Identification of virilizing adrenal tumors in hirsute women. N. Engl. J. Med. 1994;331:968–973. - PubMed
-
- Prager G., Heinz-Peer G., Passler C. Surgical strategy in adrenal masses. Eur. J. Radiol. 2002;41:70–77. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
